Did you know that your CV sucks? Well, I’m pretty sure it does. And in this post, I am going to talk to you about the most likely reasons why your CV sucks. And how to fix these problems so your CV stands out.
As a real doctor who is also a medical HR expert, I get to see a lot of professional CVs and resumes mainly from other doctors. And inevitably most of them have some real obvious faults and problems that need to be fixed up. These are simple errors that you can fix yourself which will dramatically affect the performance of this key document.
In summary, the top errors on CVs that I generally see and which result in me concluding that a resume sucks or a cv sucks are as follows:
Including a photo on a professional CV. This is an absolute no no.
Not taking the time to customise your CV to the job you are applying for.
Putting your information in the wrong order (to what the employer wants/needs).
Too many embelishments.
Typographical errors, grammatical errors and spelling mistakes.
Read on further as we discuss these problems so you can find out why your CV sucks and fix it.
Does your resume really suck? Does your CV suck?
Yes. Probably at least a little bit. It doesn’t mean that what you have written is all bad. It’s just that perhaps you haven’t looked at it from a sales and marketing perspective. Once you understand that your CV or resume is a key marketing document (i.e. it’s meant to sell you!) you will start to figure out why I am saying that your CV sucks.
Most of the clients that I work with are doctors or other health professionals. Looking at it from a professional CV perspective it’s important that you try to maximise the success rate of your CV. Or what we are really talking about here is your resume.
Your CV or resume’s main job (arguably only job) is to ensure that you get an interview for the job you applied for. If it hasn’t done that, it’s failed you. And then that CV definitely does suck.
The Number One Reason Why Your CV Sucks. Including a Photograph.
The number one problem that I see with people’s CVs is photographs. As nice as you may be able to look in a photo there are so many reasons why including one on a professional CV or resume is simply a bad idea.
I go over the reasons in more detail in this post. Or if you prefer a video watch this.
However, a key reason you want to avoid including a photograph is that it is not expected by the panel and therefore often seen as pretentious.
Another reason you want to avoid using a photograph is that it will introduce biases. Once the reader sees what you look like they can make all sorts of assumptions. Why not wait till they meet you in person so you can make a true first impression.
Finally, a photograph is distracting on a CV or resume and may just take up a few vital seconds that you would prefer that the reader use to examine the contents of your document.
Now, the inclusion of a photograph does depend on what sort of job you’re going for. But again, for the clients that I work with who are medical practitioners, professionals, it really is not accepted practice to put a photo on your CV. And therefore you should refrain from doing so.
Leaving the photo off actually gives you a bit more real estate on the front page to play with, which is the added bonus there.
So the solution is no photos on your CV.
The Second Reason Why Your CV Sucks. Not Customizing to the Job.
Now the number two problem that I see with people’s CVs and resumes and why you might hear me say your CV sucks is a failure to customize your document.
What do I mean by customizing? I mean tailoring it or adjusting it. This is something that you should do every time you go for a new job. You should be submitting a different resume each time.
You should be ensuring that that your cv represents you effectively in terms of how you are the best fit for that particular job.
This doesn’t necessarily mean that all of your cv sucks. And you don’t necessarily have to go through and edit all of the sections on it. But have a think about it. What highlights, particularly in your personal summary, do you want to put across that show that you meet the specific criteria and key challenges of that job?
And of course, the solution then is to customize your cv.
Because you may be applying for a number of jobs on a regular basis or over time. What I would actually recommend that you do, is keep a master document, a proper curriculum vitae if you will, with all of the information tracking your career over the years. That is all your jobs, all your education, all your qualifications, all your professional development, et cetera…
Then each time you go for a job, reflect on that master CV and your most recent resume and put together a new resume, which is a tailored version of these 2 documents aimed at the new job.
The Third Reason Why Your CV Sucks. The Wrong Information in the Wrong Order.
The third problem that I see with CVs and resumes is information being presented to the reader in the wrong order. Especially the wrong information being presented on the first page.
Not putting the key information that employers want to see on the first page of your resume is a sure fire way to frustrate a potential boss and be overlooked for an interview.
The first page is critical. It’s like real estate. When you understand that generally, someone is only glancing at your CV for a few seconds on the first review. This brings this particular point to home.
The first page of your resume is the thing that people first look at, and it’s the thing that recruiters spend the most time glancing over. And then they will usually hop over to the end and look at your references, and will probably skip all the stuff in the middle.
So you want to optimize the first page. It’s really valuable real estate for you from a marketing perspective, you need to know the key things that need to be on that first page. And what you can leave for other pages.
So what are the key components for the first page of your CV?
Firstly, obviously, you should have your name. And your name should be in the biggest font size on the page. Because it should be the hero of your page. And it is the thing you want them to remember.
So rather than having a photo, have your name in the biggest font size that you can comfortably fit it into on one line at the top of the document.
Next. You will obviously need some contact details. These days that really only has to be a mobile phone number and a professional email address. You can skip the postal address. They are probably not going to mail you anything.
Next. Is “key information”.
What do I mean by key information?
So again, my example here is medicine. Key information in medicine would be things like your short qualifications, i.e. MB BS or similar. Things that you must have to do the job. In some cases, this will also be specialty qualifications, like FRANZCP.
Other key information might include medical registration information (which is generally also essential for most medical jobs), as well as things like English language tests and visa status.
Put down all the key things that you know the employer is wanting to see very quickly that will help them determine whether you’re actually eligible and meet the key eligibility criteria.
After this, you should have enough room on the first page for the other two key components.
The first of these is a personal summary, which should take up around a third of the page and maybe one to two paragraphs. which is your executive summary, presenting your career your way (rather than them interpreting it from looking through the rest of the document).
And finally, but importantly, work history.
Employers want to see what you’ve been doing in your job. Remember, you’re going for a job, so they want to see what the current job is that you’re doing.
What are you achieving currently in that job? And maybe, if you’ve only been in the present job for a little while, what did you achieve in the job before that.
This is the key thing that employers want to know. What are you doing now? Who are you working for? How well are you performing currently (not 10 years ago)?
So what can I leave till the next page of my CV?
Some of the things you can leave for the next page or the one after that include things like education history, courses, professional development, and research. These are not as essential as the things I have listed above.
Sadly, sometimes I see candidates list lots of other things, such as a detailed education section, courses and certifications before we get to the work history, buried on the 2nd or 3rd page. This is really putting you at a disadvantage. And in this case, I can definitively say that your CV sucks.
So the first page is crucial to have the right information in the right order.
The Fourth Reason Why Your CV May Suck. Too Many Things Happening!
Now, the fourth and the second last tip I’m going to give you about how to fix your CV. Is to watch out for too much going on or too much happening on your CV.
Now, what do I mean by this?
This could mean many things. But common issues I see are things like:
having too many different fonts,
having too many styles,
having different bullet points,
indents not aligning,
text cramped up,
too many colours being used,
not enough use of white space,
images and icons
Things that just kind of make the document jar on you.
For a professional CV. Try to keep your CV as simple as possible.
It should look sober and fairly conservative, but be readable and still pleasant to look at.
Of course, you can still put a bit of your own sort of style into it. But less is more.
You don’t want to be overloading the reader. You want them to see the critical information that you’ve got.
What’s my solution for that?
Well, you can spend a lot of time trying to work with Word documents and templates or Google Docs. I’ve seen people recommend going into Canva, for goodness sake!
I don’t know why you would do that. Canva is good for graphic design. But very slow for long documents.
Don’t do any of these things.
Use something that’s developed to help make a very professional polished. CV easily and cheaply, which is an online CV builder.
Online CV Builders A Great Hack for How to Fix Your CV
The Fifth Reason Why Your CV Sucks. Spelling Mistakes and Typos.
You’ll be amazed how easy it is for one or two spelling mistakes and typographical errors to creep into your document. These errors can just really bring it down.
Again. If we are talking about professional or professional people going for jobs where attention to detail is critical, particularly in medicine. Errors on your CV can leave a significant negative impression.
So it’s important that your resume, or your CV, be absolutely perfect. That there not be any sort of missing dots or commas or spelling mistakes. Things that make the reader think, well this person really didn’t check this document properly, did they?
So what’s the solution to this problem?
Well, you have spent all this time putting this document together, and you have probably gone through it several times. So you are probably missing things now because you’re skimming over them.
So get someone else to check your CV or resume.
Make sure that they identify any of those spelling errors and typographical mistakes.
In addition, use the inbuilt functions of things like Microsoft Word. Or if you’ve got Grammarly for the internet use something like that if you’re working online. These programs are built to show you your errors and may even help improve the tone of your document.
This blog is open to comments, I also run a YouTube Channel and a Facebook group and frankly way too many other ways for people to contact me. So no surprise. I do get a lot of questions and queries on a daily basis. One of the surprisingly common and interesting questions that I do get a lot from doctors from other countries is “do doctors get paid to train in Australia?”. Being paid for work is part of our culture in Australia. But I am aware that in other systems you may not necessarily be paid when you train in medicine or even have to pay for your training.
So let’s try to clear up this question in this blog post. Along with answering some related questions that come up around this topic.
From the time after you graduate from medical school in Australia, you will be entitled to and will receive payment for your services as a doctor. This includes any further career stage which might be referred to under the label of training. So you get paid to be an Intern, you get paid to be a Resident and you get paid to be a Registrar (which is what most doctors who are undertaking specialty training in Australia are referred to).
Therefore, you also get paid when you are doing surgical training, physician training, psychiatry training, emergency training, general practice training etcetera. You also get paid when you become a specialist doctor or consultant, although in some cases you may be working for yourself, in which case, you are paying yourself out of the revenue you collect.
What does all of the above means for international medical graduates (IMGs)?
Do IMG Doctors Get Paid to Train in Australia?
The answer is again yes. If you are an IMG doctor and you get appointed to any training position, whether this is a resident position for the purposes of completing the standard pathway process or a specialty training (Registrar) post as part of any of the competent authority, the specialist, or the short term training in a medical specialty pathways. You will get paid.
Whilst wage theft and the exploitation of overseas workers in Australia have become a real concern in Australia over the past decade or so. I am not aware of any such situations that have involved international medical graduates. If you do know of such a circumstance I would be interested to hear from you.
Do IMG Doctors Get Paid Differently to Australian Doctors?
This is a more complicated question to answer.
As a general rule if you are an IMG doctor and you are recruited to a position you will be paid under the same classification as any Australian doctor also doing the same job. So if, for example you are appointed to a Resident position you will be paid as a Resident.
However, for most classifications, there are steps or levels that increase based on your years’ of experience. Sometimes the employer may try to start you out at the bottom of this classification scale, even though you may actually have more experience, citing that you don’t have any experience in Australia. So in this case you may end up being paid slightly less. In my experience, most employers in Australia will try to recognise your experience and pay you at a higher rate if you are eligible. This is a grey area in terms of what is correct. So it’s definitely worth querying things if you feel you are on the wrong end of the stick.
Why Do Doctors Get Paid to Train in Australia?
The answer to the question of why doctors get paid whilst training is that they are performing real and substantial services in these roles. The training is on top of this work or embedded into this work. They are generally not taking large amounts of time away from the workplace to attend things like lectures and seminars or workshops. Much of the training occurs within the workplace and a lot of the additional studying occurs in the doctor’s own time after work.
Many Doctors Do Have to Pay to Train
Hang on. What’s that? You just said that doctors get paid to train. But now you are saying they also have to pay?
Doctors do get paid to train in Australia. But there are some costs associated with being a trainee doctor in Australia.
There are the normal regular costs like paying your medical registration every year and having a car so you can get to work.
But there are also some specific costs associated with being a trainee doctor.
As an intern, you generally won’t have any particular costs associated with your training as it will normally be provided for you by the hospital.
As a resident doctor, you will probably be thinking about paying for some courses that might help you get into a particular training program. So things like emergency courses and anatomy courses and radiology courses and the like.
As a specialty trainee doctor, you will have to pay college membership fees, you may also have to pay for a formal education course and you will have to pay to sit examinations.
Personal costs for training as a trainee doctor in Australia can rack up to several thousand dollars and even pass into the tens of thousands of dollars range. But this is generally over a significant period of around 5 to 10 years.
We are approaching that time of the year again in Australia. The time where the majority of trainee doctors go up one step of responsibility on the ladder. It’s also the time that our newly graduated medical students commence their first paid position as a doctor. Commonly referred to as the internship. You might be keen to know how much you are going to be paid and how this compares to other States and Territories. How much do interns make? You may be surprised how much it actually varies.
Interns across Australia are paid according to State or Territory based Awards or Enterprise Agreements. The annual rate of Intern pay varies considerably with NSW Interns being paid the worst and Western Australian Interns being paid the best. In order of ascending annual Intern salaries are as follows: New South Wales $71,283, Tasmania $73,586, Australian Capital Territory $74,826, South Australia $77,084, Northern Territory $78,757, Queensland $78,941, Victoria $79,138, Western Australia $79,479
NSW
Tas
ACT
SA
NT
Qld
Vic
WA
$71,283.00
$73,586.00
$74,826.00
$77,084.00
$78,757.00
$78,941.00
$79,138.09
$79,479.00
as of Jul 2021
as of Jul 2021
as of Dec 2020
as of Apr 2020
as of Jan 2021
as of Jul 2021
as of Jan 2021
as of Oct 2020
as of the latest publicly available Award document or equivalent
How Much Do Interns Make? There Is A Wide Variation In the Entry Doctor Pay Rate
The results above reveal that there is a wide variation of $8,196 or a 9.5% difference between the lowest paid annual salary and the best paid annual salary. Interestingly this gap has closed somewhat since we looked at it a couple of years ago.
The reason for the large variation is that each State and Territory sets its wages for public employees separately through something called an Award or an Agreement. These are formal documents that state the conditions of employment. They include matters such as the hours of work, the leave available and of course how much you get paid.
These Awards or Agreements are generally only comprehensively reviewed every few years at best. In the meantime State and Territory governments generally negotiate with the employee’s unions for an across the board annual wage increase somewhere around the rate of inflation.
Doctors like other public employees do not generally contract as individuals for their services with hospitals. So everyone gets the same conditions based on what role they are employed in and what year they are at.
According to the Australian Bureau of Statistics Full Time Adult Average Annual Ordinary Earnings was $93,729 in 2021. So bearing in mind that it takes a minimum of 5 years of university study (with a fair collection of higher education debt to pay off) to get to this point we can certainly not consider Interns to be extremely well paid.
But it’s not all that doom and gloom. Whilst, Interns certainly do not work the amount of overtime they used to 10 or 20 years ago. Overtime provisions, as well as loadings (working rostered hours on an evening, night or weekend) under most Awards and Agreements, can lift the annual take-home pay of an Intern significantly. For e.g. most overtime starts off being paid at 150% and rapidly goes to 200%.
So, if we take this into account when asking the question how much do interns make. If an Intern works on average 50 hours per week they are likely to hit Full-Time Adult Average Annual Ordinary Earnings, even in a State such as NSW.
An additional bonus for Interns comes at the first tax time. In Australia, the Financial Tax Year runs from July to June. So, because you have not been paying much in the way of taxes for the first half of the financial year, you end up paying more tax than you need to in your first 6 months of Internship and get a reasonable return come tax time. For this reason, some Interns seek to work extra overtime before 30th June.
What’s Going On in NSW?
NSW has the highest number of intern positions in the country. So it may be that you came to this blog post wondering how much do interns make in NSW.
When I was an Intern, NSW paid some of the best salaries for trainee doctors in the country. States like Western Australia (which is now first) were actually towards the bottom of this list.
Given that NSW is the biggest State in Australia by population and one of the richest States economically. And given that Sydney (NSW’s capital city) is probably the least affordable place in Australia to live it makes little sense that NSW Interns get paid the least.
It’s hard to know exactly why this situation has occurred. It is possible that the industrial groups that represent doctors in other States and Territories have been more successful in representing trainee doctors over the years.
This certainly seems to be the case if one looks at the Enterprise Agreement for doctors in Victoria. Which even includes an allowance for continuing medical education, as well as separate provisions for internal training leave, examination leave and conference leave.
So whilst the question of how much do interns make is an important factor in determining which State or Territory is the best to be an intern. We do need to take into consideration a range of other factors.
It’s that time of the year again in Australia for the medical system. The time where around 90% of the trainee doctors in the health care system step up a level in responsibility. And it’s all done in a matter of a few weeks from mid-January to early February. This includes all the new graduated medical student doctors who are commencing their first paid role in the system as interns.
Add into this equation the current additional pressure being experienced on our health care system due to increasing COVID-19 cases it is even more important to have good systems in place to ensure that doctors taking on new levels of responsibility are appropriately supported. If your formal orientation and onboarding system does not include a well thought out buddy program then it should.
So here are my 7 top tips for a successful buddy program in medicine:
Have a checklist
Get the buddies to write the checklist
Sell the buddies on the personal and organizational benefits
Have a clear exit date for the buddy relationship
Support your buddies through the program
Give guidance about how often buddies should meet with their new doctor
Troubleshoot problems with the program if/as they emerge
Read on further to find out more about what exactly is a buddy program in medicine, how it can complement and benefit a hospital’s formal orientation and onboarding system and a more detailed explanation of my key tips for a successful program.
What is a Buddy Program?
Buddy programs have been used in a range of industries and educational settings for many years and are proven to be effective ways of ensuring that employees/students get off to a good start. This has all sorts of benefits to both employee/student and the organisation.
Simply put a buddy program involves assigning a new employee a workplace buddy. For a buddy program in medicine, the buddy is an existing doctor who guides the new doctor through the first few weeks or months on the job.
In Australia we have started to see the rise (or in some cases rebirth) of buddy programs, sometimes also referred to as mentor programs. In particular, it is now common in the State of NSW, for the second of the 2 weeks of Intern induction to consist of a “buddy week”, where the new intern gets the chance to understudy a finishing intern in their first new rotation.
Whilst these buddy weeks are quite popular they do have their limitations. The key one is that because the relationship is very brief it only really permits a small transfer of knowledge and in particular doesn’t afford the new intern doctor a chance to reflect and ask questions of their buddy about the “hidden curriculum” of the workplace.
Evidence has emerged that longer relationships between new employees and existing employees in Medicine can help reduce stress and improve morale, sense of support and job satisfaction.
Tip Number 1 For a Succesful Buddy Program in Medicine – Implement a CheckList
Buddy programs in medicine should include a formal documented process that outlines the buddies’ responsibilities as well as what items they should cover over the first few weeks or months of employment. The buddy program should also encourage the buddy to share with the new employee to share tips, tools, knowledge, and techniques they have learned about the workplace.
The documentation does not need to be lengthy or complex. It can be as simple as a one-page checklist.
In fact, here’s an example of a buddy checklist I once implemented in my own hospital setting for new interns in mental health that was very successful.
Topic
Completion Check
Has downloaded Med App and is able to login and access
Knows where to find things in the Med App
Tour of Ward
Tour of Hospital
Introduced to Team
Introduced to Consultant
Introduced to Registrar
Introduced to NUM
Has Term Description
Access to Resources on Shared Drive
Duress Trained and Aware. Knows not to actively participate in a Code Black (PMVA) restraint – need to be trained (It’s OK to go fetch the patient’s notes and med chart and be available)
Knows when education is and where and where to find the topic list in RG
Knows how to get a patient list
Can access email and Clinical Applications
Has read weekend After Hours Roster and understands weekend After Hours responsibilities
Can complete a Discharge Summary
Can complete a Tribunal Report
Knows how to contact the community team
Knows how to request pathology and imaging
Knows how to obtain drug levels and withhold morning medications if necessary
Knows not to prescribe Clozapine till registered
Run through any MedChart, EDRS, IIMS, CAP etc… #hacks that you have found useful
Can write a schedule and Form 1
Knows role in the ward round
Can describe the roles of other team members (e.g. Consultant, Registrar, NUM, ward clerk, nursing staff, psychology, social work, occupational therapy etc…)
Has visited the library and can access CIAP
Knows where to lookup drug information (e.g. eTGA, UptoDate)
Understands process for dealing with a Medical Emergency (MET) call
Understands process for dealing with a deteriorating patient
Understands process for requesting a medical or surgical consult
Understands how to request/arrange a rostered day off
Why Implement a Buddy Program?
The last thing we should hear from a doctor on their first day is “Nobody knew I was starting today.” At the end of their first few weeks in the job, we want new interns to feel that they made the right decision to study medicine and for other doctors starting new jobs we want them to feel that they accepted the right position.
First impressions are key. The initial enthusiasm that interns experience to have “finally made it” can be either lifted or ruined, depending on their start.
Regardless of whether there is a formal process in place or not, onboarding is going to happen. The real issue is the quality of the experience. When onboarding is done well it sets up new doctors for long-term success. If an orientation simply consists of handing the new intern a pile of forms to fill out on their first day, then there are going to be future problems, which is where a buddy program may come in handy.
Implementing a buddy program in medicine can be part of an effective onboarding program that provides new doctors with a way of resolving questions regarding work processes. Some of which may be difficult to predict and/or hard to deal with in a formal orientation seminar. This socialization and support can make a big difference.
Well executed buddy programs complement the existing formal orientation talks and employee handbooks by allowing the new doctor to ask questions of an expert (the buddy), to make sense of the information they have received and address gaps in information that the orientation program has not identified.
They also allow for a transfer of “real-world” knowledge that would be difficult to do in a handbook or orientation seminar. Buddies are better situated to deal with the “profane” aspects of the workplace, the hidden rules and processes.
Tip Number 2 For Implementing a Successful Buddy Program in Medicine – Get the Buddies to Create the CheckList
Buddies are the real experts in how to do the job. Because they have been living it and doing it for the past year or so. They are therefore better situated to create a more effective checklist for the buddy program because they can still remember the things that they found difficult or surprising to do in the first few weeks.
To do this I recommend sitting down with your prospective buddies a few weeks out from the transition and engaging them in a discussion about being a potential buddy. Explain what you are seeking from them (see below) and then ask them to help you generate a checklist.
By all means, have a list of things you might think are important. But be prepared to alter this based on the buddies feedback.
Here’s a classic example.
When I was an intern (many moons ago now) it was quite common for interns to have one or two small books that they could carry around with them in their pocket as reference guides for how to deal with certain clinical situations.
When I was putting together my own buddy program in medicine, I asked my potential buddies what sort of books they would recommend to new interns to buy. The buddies uniformly told me that they would not recommend purchasing a book either in a physical or digital format. Instead, they recommended that new interns use the Med App* that their hospital had purchased for them that had a wealth of information curated for them and tailored to local needs.
Tip Number 3 For Implementing a Successful Buddy Program in Medicine – Sell the Buddies on the Benefits of the Program
The buddy program in medicine is not only valuable to the new doctor. Its obviously also an opportunity for existing doctors to develop skills as a mentor and may foster the early development of a range of people management and leadership skills.
From a bottom-line point of view, a well-executed buddy system will likely reduce the number of doctors leaving a hospital or organisation, particularly early. And this will save the hospital a lot of money in re-recruitment costs. But it also means to the buddy that they are investing in a stable workforce that means they are less likely to need to step in to fill gaps on the roster.
At a deeper level, buddy systems can improve employee engagement with the organisation which can be a vital component of instilling a positive workplace culture. Which in itself is likely to lead to better outcomes in terms of both patient care and cost.
Benefits To Buddy
Benefits To New Doctor
Recognition
One-on-one assistance and single point of comfortable contact
Expand Network
Jumpstart on networking
Opportunity To Lead
Smoother acclimation
Fresh Perspective
Knowledge of “how things really get done”
Tip Number 4 For Implementing a Successful Buddy Program in Medicine – Have a Clear Exit Strategy
Hospitals and health care networks are busy spaces and constantly changing. Rosters are open to disruption. On a practical level, it’s likely that your buddy and their new doctor pair only have a limited time when they will be in the same location before one or the other might be working somewhere else.
Buddies may be worried about the commitment you are asking for.
So I recommend being clear about this issue in your discussion with both the potential buddies and new doctors. I recommend asking for a minimum one-month commitment from your buddies. This will usually permit an intense initial one-week buddying experience followed by some regularly weekly catch-ups to address any ongoing gaps.
Who Makes a Good Buddy?
A buddy is someone who partners with a new doctor during their first few weeks or months of employment. He or she is a colleague assigned to assist the new doctor to get through this period. They can provide insight into the daily activities of the hospital and help the new doctor fit in more quickly.
A buddy also potentially gives the new doctor a psychologically safe opportunity to offer confidential feedback about how their onboarding process is going. For these reasons the closer the buddy is to the new doctor in terms of peer relations the better.
An effective buddy is a good communicator, has an interest in the development of others and is the type of doctor the organisation hopes to emulate (fits with the value system). They will generally take the new doctor around their hospital and orientate them and introduce them to key people who can help them out.
Tip Number 5 For Implementing a Successful Buddy Program in Medicine – Choose Good Buddies and Support Them
A Good Buddy
Is known as a good performer and well regarded;
Is willing and able to mentor others;
Has the time to be available;
Knows the new doctors job;
Is a peer of the new doctor;
Has good communications and interpersonal skills.
A good buddy should be a good representative of the culture and values of the hospital and organisation and be familiar enough with the formal and informal organizational structures to be a reliable source of information.
Buddies Should Not Be
A buddy is definitely not a supervisor and probably should not be a mentor (at least in the first few months). This helps to make the task of the buddy more limited and definable.
Learning how to be an effective buddy can be useful as a foundation step to learning how to be a mentor or supervisor. The buddy is are available to answer straightforward questions about how the hospital operates. It is important to make clear to both the new doctor and the buddy that the buddy is not being asked to develop the new doctor and is not accountable for performance. This makes the buddies role easier in terms of being able to support the new doctor without fear of reprisal.
If a doctor does not want this extra responsibility, then they should not be assigned the buddy role. Some doctors simply don’t want the responsibility or are not ready.
Worse, some doctors are not well suited temperamentally for the role. A doctor who is known to be someone who gossips at work is probably not a good fit for a buddy role. The last thing a new doctor wants to hear about is gossip and speculation in their first few weeks.
For a successful buddy program in medicine, buddies should have the skills and knowledge to be able to:
Teach or tutor, for e.g. explain an unfamiliar task;
Explain tactical matters, such as how to submit a time-sheet and where the pathology forms go;
Talk about and explain the hospital’s structure, written as well as unwritten rules;
Share insights on how things are done in the hospital;
Involving the new doctor in social activities, such as coffee and lunch with new team.
In my experience, most doctors who put their hand up to be a buddy already have these skills for the most part. But they may still be somewhat anxious about whether they are doing a good job.
Buddies can benefit from some training and support in their role. But probably the best thing that can be provided is a suggested list of tasks and a timeline for completing them as I have highlighted above.
As part of your succesful buddy program in medicine, I recommend scheduling regular sessions with your buddies throughout the timeframe of the buddy program so you can support them, find out how the program is going and help troubleshoot any issues. This can normally be done as a group meeting.
Tip Number 6 For Implementing a Successful Buddy Program in Medicine – Give Guidance About How Often the Buddy Should Meet With the New Doctor
Generally speaking, the buddy is encouraged to meet more frequently with the new doctor e.g. daily for the first week, weekly for the first month, monthly for the next few months and formally exit from the relationship.
For your particular buddy program in medicine, it is helpful to set a solid time frame for when the relationship finishes. A month is okay, 3 months is good, 6 months is great if you can manage it.
Emphasise to your buddies that during the first few meetings that they should work to help with urgent and practical questions. As the relationship matures and the new doctor finds their feet the explaining turns into more of the “why things are done this way around here.”
Tip Number 7 For Implmenting a Succesful Buddy Program in Medicine – Troubleshoot Problems With Buddy Programs
There are some practical problems with buddy programs in medicine, particularly when assigning buddies in hospitals. Firstly, there are often not enough experienced buddies to go around. Especially if you have 100+ new interns starting all at the same time. Secondly, often those who are identified to act as buddies are taking leave or moving on at the same time as when the new doctors are arriving.
One way to get smart about this issue is to gather information and consider the level of readiness of the new doctors. There are likely to be some in this group that require more support than others. Typically some may have already studied at the hospital as students or worked in the hospital already and have a level of familiarity. These new doctors can probably more safely be assigned less experienced buddies and you can save your best buddies for the completely new doctor.
As part of your buddy program in medicine, set up regular training and check-ins with your buddy group can identify gaps and issues. This can be triangulated with sessions with the new doctors themselves.
Tips for Being a Buddy
If you are asked to be a buddy, here are some tips that can help you:
Keep a list and timetable of what things the new doctor needs to know or be shown;
Be patient. Relationships take time to develop. Your new colleague is unlikely to open up to you until they have spent a bit of time getting to know you and you have earnt their trust;
You are not the expert on everything, instead think about who else can answer questions you don’t know the answer to and introduce them to the new doctor;
Don’t try to cover everything at once. Remember the new doctor is going to feel overwhelmed in the first few weeks. So try to avoid cognitive overload. Leave the deeper discussion till later;
Stay positive. New doctors will grow into their roles in time with appropriate support and confidence is infectious. Maintain a positive, teaching attitude;
If possible try to identify the new doctor’s personality and communication style and adapt;
Be open and don’t judge. Your new doctor is relying on you to be a safe place to get answers to their many questions.
Remember. Despite the best efforts of the manager who asked you to be a buddy. Sometimes buddy relationships don’t work out. Don’t be afraid to approach your manager to express concern and/or suggest an alternative buddy.
Summary
Creating a buddy program in medicine for new doctors requires some time investment and buddy choice should be carefully considered. However, this is not a difficult or expensive option to implement.
Make sure you’ve chosen a willing and effective buddy; create some documents to support them and the new doctor. Set an end date for the formal buddy relationship. Watch for the things that do not work so you can guide both the experienced and new doctors.
A buddy system can dramatically reduce the time a new doctor requires to be productive and aid retention. An additional benefit of a buddy program is that it allows for corporate knowledge sharing and positive recognition for the buddy.
Related Questions
What’s the Difference Between Buddying and Mentoring?
There are a number of key differences between buddying and mentoring. The relationship in buddying tends to be more superficial, social and focused on helping to solve immediate problems. The time frame of a buddying relationship is generally more limited than in mentoring. As a buddy, you may be asked to work with your new colleague for a week to a few months. In contrast, mentoring relationships in medicine tend to last for many months and generally years. The relationship, therefore, becomes deeper over time and is focussed on the mentor imparting their knowledge and experience to the mentee to assist the mentee in their development in their role.
*The author declares that they are an investor in Med Apps the company that produces the Med App Application.
Of all the medical specialties surgeons have the reputation of being the most confident and competitive. At face value, these are traits you would definitely want to have for someone operating on you. So it’s not surprising that the process to become a surgeon in Australia, or gaining entry into surgical training is one of, if not the most, competitive processes in medicine. In this post and guide, we will take you through the key steps in becoming a surgical trainee, including looking at what information exists in relation to competition ratios.
In summary, in order to become a surgeon in Australia, you must first compete to gain entry into a medical school program, graduate and complete an internship year. You will most likely spend several years working in RMO, Senior RMO and unaccredited posts whilst accumulating experiences that count as points towards your application, learning the basics of surgery and perfecting your interview technique. If your application is deemed sufficient, once per year you will be invited to participate in the Surgical Education Training selection interviews for one of the 9 surgical subspecialties that make up the Royal Australasian College of Surgeons. The interviews are all structured and generally of the Multiple Mini Interview format. Acceptance rates vary by specialty and from year to year but your chances of getting accepted range from between about 1 in 5 to 1 in 4, making it important that you have a Plan B.
Becoming a surgeon definitely presents a great vocation. Surgeons generally attract the highest incomes amongst the medical profession (and in fact amongst all Australians). But the downside of this can be the number of hours you need to put in per week. Not just part of training but afterwards.
So let’s take a deeper look into the process. Starting with the preliminary steps you will need to undertake if you wish to become a surgeon in Australia.
Get Help with your SET Interview Preparation
If you are appearing for the RACS SET Interview you can get some help and early assistance by attending our free webinar where Anthony takes you some of the tips and techniques he has used with past clients who have had success in their application.
Gaining entry into medical school. Your first step in the process to become a surgeon in Australia.
In the old days, your local barber was also your surgeon. And you learned the “trade” by being an apprentice. However, nowadays you can’t just directly apply to become a surgeon. You must first go to medical school.
You can do this directly out of high school as part of an undergraduate program of study which will take you 5 to 6 years or a little bit later in life after completing another degree as part of a postgraduate program, which will take you 4 years (plus the years for your first degree).
Gaining entry into medicine is competitive in itself and medical programs in Australia have the lowest offer rates for students (i.e. the number of students applying versus who gets in is the highest).
For example, according to this article. 3 particular medical schools in 2020 had a combined number of 9,000 applications for 458 places. So only 5% of applications received an offer.
Does it matter which medical school you go to if you want to become a surgeon in Australia?
One question many high school students have is: does the medical school that you go to influence your future career.
The simple answer and truth to this question is not a great deal. You see all medical schools are accredited by the same body (the Australian Medical Council) and therefore at the end of the day produce the same quality of graduates. As an experienced medical recruiter, I have never really been all that bothered about where a particular doctor did their medical school.
The main purpose of completing a medical degree is to gain an internship offer. And because, by and large, all Australian medical school graduates do gain an internship offer (most are guaranteed one) no one really focuses on your medical school background as there is very little point in doing so.
So where you go to for your medical school does not matter. But what you do during your time at medical school can matter.
Are there things you can do in medical school in order to improve your chances of entry into surgical training?
There are definitely some things you can do during medical school to advance your prospects of gaining entry into surgical training. Many medical students are quite focused on becoming a surgeon from an early stage.
So if that’s you. You will probably want to look ahead and review both the general selection requirements for surgical training as well as the specific requirements for certain specialties. And then think about how you might be able to accomplish some of these whilst during medical school.
For example, for most of the RACS SET training applications points are awarded for items such as academic excellence, teaching and mentoring, rural and remote experience and research experience.
In addition, a lot of medical school programs will have surgical interest groups or extra opportunities to experience surgery as part of medical school. Engaging in these opportunities will not only enhance your knowledge of surgery but also provide the opportunity to establish mentoring relationships with current surgical trainees and even consultant surgeons.
Now. If you have already come to the end of your medical school training and feel like you may have missed out on some opportunities. Don’t fret. There’s plenty of time still to prepare.
The Prevocational Years.
After completing medical school in Australia or New Zealand you will be required to complete a mandatory provisional year or internship in order to obtain general registration. As part of this year, you will generally be required to undertake at least 10 weeks of experience in a surgical role. Whilst this post may give you some exposure to the operating theatre you are likely to spend most of the time on the wards admitting patients prior to operations and assisting in their postoperative recovery.
After completing an internship it is quite rare to be able to gain a role working entirely in surgery so most trainee doctors who want to apply for surgical training will undertake a second general year which is normally referred to as a resident medical officer role. In this year you may be lucky to gain more than one term in surgery.
The Postgraduate Year 1 and 2 years are commonly referred to as the “prevocational” training period in Australia and New Zealand, i.e. the time after medical school and before entering into specialty training.
There are lots of ways that you can maximise your prevocational years if you are intending to apply for surgical training. These include:
gaining as much experience in surgery as possible during this time;
ensuring that when you are on a surgical term you manage your ward patients effectively and efficiently so that you learn about perioperative care and so that you are invited to theatre by registrars and consultants;
attending theatre when able, which will generally include you having an opportunity to assist as a third pair of hands or occasionally as the primary assistant;
making the most of your other rotations to acquire knowledge and learn skills relevant to surgery (there are some terms that make a lot of sense if you want to do surgical training, for e.g. emergency, anaesthetics and intensive care, but don’t underestimate how much you can learn from a medicine term or even a psychiatry term);
attending local surgical clubs;
offering to assist the local medical school in tutoring in surgery and related areas such as anatomy;
completing relevant and required courses (see below);
developing mentoring relationships;
participating in surgical audits; and
participating in surgical research.
The Unaccredited Years.
It is important to note that many trainee doctors spend several years in various SRMO and unaccredited registrar roles without gaining entry into SET training. During this time there is no official training body representing your interests so you may be more open to exploitation. The cautionary tale of Dr Yumiko Kadota shines a light on some of the problems that may confront you.
Most wannabe surgical trainees will use these years to continually improve on their application for surgical training and prepare for the selection interviews which are held once per year.
They will attempt to accumulate as much surgical experience as possible, including operative experiences and will generally keep a logbook.
It is also at this stage that most trainees will settle on a particular surgical specialty of choice and attempt to gain the most experience and knowledge in this particular specialty.
The 9 options are:
Cardiothoracic Surgery
General Surgery
Neurosurgery
Orthopaedic Surgery
Otolaryngology (ENT)
Paediatric Surgery
Plastic and Reconstructive Surgery
Urology
Vascular Surgery
Preliminary Requirements for Surgical Training.
The process for applying for SET training begins early every year.
Anyone intending to apply for SET selection must first register their intention to apply within the specified time frame, normally in January of each year. At the time of registration, applicants must be able to meet all generic eligibility requirements (see below). A registration fee of $595AUD must be paid by any applicant who is not a current SET Trainee or RACS Fellow. All registrations are conducted online through RACS. This fee is in addition to your application fee.
According to the Royal Australasian College of Surgeons which governs surgeons and surgical training in Australia and New Zealand there are a number of general requirements that you will need to have in order to apply for surgical training.
Firstly, anyone wishing to apply to surgical specialty training in Australia must have Australian citizenship or permanent residency and General Registration.
Secondly, applicants must also complete a RACS specific Hand Hygiene Learning Module and the RACS Operating with Respect eModule to submit with their application.
The final generic eligibility requirement for the RACS is passing the General Surgical Sciences Exam (GSSE), an exam covering anatomy, pathology and physiology costing $4145 to sit in 2021.
Trainee doctors who register for SET selection and are confirmed as satisfying the generic eligibility requirements may then lodge an application for selection from the specified date in February or March.
Specific Requirements for SET Training Schemes.
All SET training schemes have additional prerequisites which you must meet in order to be able to apply.
As an example, to apply for cardiothoracic training applicants must have had a minimum of 2 surgical terms of at least 10 weeks duration in any surgical specialty in the past 6 years, plus a minimum 10-week rotation in cardiothoracic surgery (this cannot be just cardiac or just thoracic).
Applicants must also have proof of competency for the procedural skill of inserting a chest drain, as well as for harvesting a long saphenous vein and harvesting a radial artery.
The Application Process.
All SET training schemes generally require an application process where your CV and referee reports are scored and this determines whether you progress to the interview phase.
You apply separately for each SET training scheme you are interested in. Just to repeat your 9 options are:
Cardiothoracic Surgery
General Surgery
Neurosurgery
Orthopaedic Surgery
Otolaryngology (ENT)
Paediatric Surgery
Plastic and Reconstructive Surgery
Urology
Vascular Surgery
In general, a percentage is applied to scoring your application and CV, as well as a percentage applied to scoring referee reports. Depending on the specialty these scores may or may not be combined with the interview score at the end. But the interview tends to attract the most weighting…
As there are generally many more applicants than training positions the application and referee scores from all applicants will normally be combined to determine who will be invited to interview.
In 2021 RACS introduced a Situational Judgement Test (SJT) as part of their selection criteria. This was mandatory to complete for application to any of the surgical specialties, however as it is newly implemented the results of SJT test did not impact on application results for 2021. The RACS SJT is apparently designed to test the domains of the RACS competencies of professionalism and ethics, Management and Leadership, Collaboration and Teamwork, Communications, and Health Advocacy.
Entry Requirements for Specialty Training in Cardiothoracic Surgery
Applicants to the cardiothoracic surgery training program are required to have specific experience prior to application. Within the last 6 years, the applicant must have had a minimum of 2 surgical terms of at least 10 weeks duration in any surgical specialty, plus a minimum 10-week rotation in cardiothoracic surgery (cannot be just cardiac or just thoracic).
Applicants must also have proof of competency for the procedural skill of inserting a chest drain, harvesting a long saphenous vein and harvesting a radial artery.
The referee requirements for cardiothoracic surgery training is for 12 total referees who are specialists and have been your supervisor in the past 4 years. At least 2 must be from the most recent cardiothoracic rotation, at least 1 from the rotation the applicant is currently on, and at least 3 from rotations in either anaesthesia, cardiology, oncology or respiratory medicine where the referee had clinical interaction with the applicant for at least 3 months.
The application fee is the RACS selection processing fee of $825.
Entry Requirements for Specialty Training in General Surgery
The General Surgery Australia (GSA) website describes the role of a general surgeon as a surgeon who, “is trained to provide expert treatment across a broad range of emergency and planned surgical procedures”.
The minimum experience requirements for entry to General Surgery includes 26 weeks of General Surgery in rotations of at least 8 weeks, and 8 weeks of critical care experience in a single rotation.
As well as this experience, applicants must also provide proof of competency in the areas of common procedural skills and professional capabilities. GSA provides a document listing all 26 skills and capabilities and requires applicants to get surgical consultants to sign the applicant off as competent in all skills and capabilities to be eligible for training. More information about which specialty rotations can be used for general surgery and critical care rotations, and the list of procedural skills and professional capabilities at the link below.
Referee requirements for General Surgery SET involve 6-10 surgical consultants who have directly supervised you as an applicant during their eligible surgical rotations. Included in this must be at least 2 specialist General Surgeons. All applicants must also pay the General Surgery Selection fee of $935 to be eligible for selection into training
Entry Requirements for Specialty Training in Neurosurgery
The role of a specialist neurosurgeon according to the Neurosurgical Society of Australasia (NSA) is to “treat conditions and diseases related to the brain, spine and nervous system.”
Applicants are allowed a maximum of 4 attempts at selection into the NSA training program. For entry into the specialty neurosurgery SET applicants are required to have 24 weeks FTE of direct neurosurgical experience within the 3 years prior to application.
Applicants must pay the $985 selection application fee prior to the application closing date. This fee pays for the neurosurgery anatomy examination which must be attempted prior to selection and a score over 70% must be achieved to pass.
Referee requirements for neurosurgery SET require the reporting of every neurosurgical specialist who has been a direct supervisor of the applicant in the previous 3 years. 3 of the specialists will be selected at the NSA’s discretion to provide a referee report.
Entry Requirements for Specialty Training in Orthopaedics
The Australian Orthopaedic Association (AOA) describes an orthopaedic surgeon as “a medical doctor with extensive training in the diagnosis and surgical, as well as non-surgical, treatment of the musculoskeletal system.”
Applicants are allowed a maximum of 3 attempts at selection into the AOA training program. The experience requirements for specialty orthopaedic training involve a minimum of 26 weeks FTE orthopaedic surgical experience within 2 years of application, made up of rotations of at least 6 weeks duration. Experience must be completed during PGY 3 or later.
All applicants must also complete a Radiation Safety Course, licenced in the state of their application.
The referee requirements for AOA SET involve providing a ‘departmental referee report’ from all orthopaedic rotations completed in the past 2 years. The ‘departmental referee report’ is a single report per rotation completed involving the opinion of the surgical team and non-surgical colleagues working with the applicant during the rotation.
The Selection Application Fee of $1,480 must be paid prior to the application due date.
Entry Requirements for Specialty Training in Otolaryngology
According to the Australian Society of Otolaryngology Head and Neck Surgery (ASOHNS), otolaryngologists are “specialist surgeons who investigate and treat conditions of the ear, nose, throat, and head and neck”.
Applicants are allowed a maximum of 4 attempts for selection into the ASOHNS training program. The minimum experience requirements for application include 10 consecutive weeks in otolaryngology and 20 weeks of surgical experience completed in rotations of at least 10 weeks duration, completed 1 January 2019. Applicants must also have completed a rotation of at least 8 weeks duration in both a dedicated Emergency Department, and a dedicated Intensive Care Unit, but these rotations can be completed at any time from the first year post-graduation.
Application processing fee of AUD $900 must be paid before the application due date.
The referee requirements involve a minimum of 8 and a maximum of 12 referees who must all be surgical consultants who have directly supervised the applicant during a rotation of at least 10 weeks. All specialist otolaryngologists who have been supervisors during the required otolaryngology rotation must be included for reference.
Entry Requirements for Specialty Training in Paediatric Surgery
The Australian and New Zealand Association of Paediatric Surgeons (ANZAPS) website describes paediatric surgery as “the specialty that includes surgeons who have specialist training in the management of children who have conditions that may require surgery. Specialist paediatric surgeons manage non-cardiac thoracic surgery, general paediatric surgery and paediatric urology. Their responsibilities include involvement in the antenatal management of congenital structural abnormalities, neonatal surgery and oncological surgery of children.”
The minimum experience requirements for the paediatric SET program involves 26 weeks FTE experience in any surgical specialty working at a registrar level, and at least 10 weeks of FTE experience in a paediatric surgery unit. Both must have been completed within the 3 years prior to application.
Applicants must also show competence in a range of procedural skills and professional capabilities to be eligible for selection. These skills are recorded in a report provided by RACS which included 27 skills that applicants must get signed off by a surgical consultant who has supervised the applicant on a surgical rotation in the past 3 years.
The referee requirements for the paediatric SET involves the submission of all supervising surgical consultants from all surgical rotations in the past 2 years, and from all paediatric surgical rotations at any time post-graduation. The selection board will then contact 3 consultants from this list for reference.
The application fee is the RACS selection processing fee of $825.
Entry Requirements for Specialty Training in Plastic and Reconstructive Surgery
The Australian Society of Plastic Surgeons (ASPS) describes the role of a plastic surgeon on their website as, “a broad scope of practice from procedures to improve your aesthetic appearance to reconstructive surgery.”
Applicants are allowed a maximum of 3 attempts for selection into the ASPS training program.
The experience requirements for eligibility involves 3 specific rotations. The first is an Emergency Department or Intensive Care Unit rotation for a minimum of 8 weeks FTE completed at any time post-graduation. Second is a rotation with direct experience in Plastic and Reconstructive Surgery for a minimum of 10 weeks FTE at any time from first-year post-graduation but within 5 years of application. The final is a surgical rotation in any surgical specialty for a minimum of 26 continuous weeks, completed at post-graduate year 2 or later, but within 5 years of application.
The Plastic and Reconstructive Surgery SET program requires a reference from 3 to 5 consultant surgeons, with direct contact with the applicant, from every surgical rotation of any surgical specialty completed in the past 3 years. It requires at least 1 reference from a clinical nurse who has worked directly with the applicant, for each surgical rotation of any surgical specialty completed in the last two years prior to application. It also requires a reference from all consultant Plastic and Reconstructive Surgeons from the most recently completed Plastic and Reconstructive Surgery rotation.
An application fee of $860 must be paid at the time of application.
Entry Requirements for Specialty Training in Urology
The Urological Society of Australia and New Zealand (USANZ) describes the role of a urologist on their website as “surgeons who treat men, women and children with problems involving the kidney, bladder, prostate and male reproductive organs. These conditions include cancer, stones, infection, incontinence, sexual dysfunction and pelvic floor problems.”
The minimum experience requirements for eligibility for an application involves 26 weeks of Surgery in General at PGY2 or above, a further 26 weeks in Urology at PGY 2 or above and 10 weeks in Emergency medicine at PGY 1 or above. All experience must be completed in rotations of a minimum of 6 continuous weeks. The Surgery in General requirement can only be met on a surgical rotation in the specialties of General Surgery, Acute Surgical Unit, Breast and Endocrine, Colorectal, Surgical Oncology, Transplant, Trauma, Upper GI/Hepatobiliary, Vascular Surgery, Paediatric Surgery or Urology (cannot also count as the urology specific rotation).
Eligibility for an application requires references from 8 consultants and 6 allied health professionals. The consultants must have been direct clinical supervisors during any rotation in the last 3 years, they can be surgical or non-surgical consultants. Of the 8 nominated, 6 are the primary referees and 2 will be reserve referees. No more than 3 consultants nominated as primary referees can be from rotations undertaken during the same year. The allied health references are divided into 4 primary referees and 2 reserve referees. Eligible allied health is ideally a senior nurse with direct and regular clinical interactions with the applicant during a rotation, though other allied health professionals can be nominated if there is proof of significant clinical interaction between the nominated referee and the applicant.
An application fee must be paid before the application due date. There is no current indication of the cost of this fee.
Entry Requirements for Specialty Training in Vascular Surgery
The Australia and New Zealand Society for Vascular Surgery (ANZVSV) describes Vascular Surgery as “a specialty of surgery in which diseases of the vascular system, or arteries and veins, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The SET Program in Vascular Surgery is designed to provide trainees with clinical and operative experience to enable them to manage patients with conditions that relate to the specialty”.
The experience requirements for Vascular surgery involves 8 weeks of General Surgery, 8 weeks of Intensive Care, and 16 weeks of Vascular Surgery completed within the last 5 years prior to application. Experience can be completed in no more than two rotations for each requirement, and rotations must be at least 4 weeks in duration. The Vascular Surgery rotation must have at least 2 specialist Vascular Surgeons employed at the hospital to be eligible.
The referee requirements for the ANZVSV training program is a minimum of 7 and a maximum of 10 supervising surgical consultants, with at least 2 being Vascular Surgery Consultants. At least 1 and a maximum of 3 referees must be nominated from each surgical rotation listed on the application.
An application fee must be paid before the application due date. There is no current indication of the cost of this fee.
Gaining “Points” in order to Become a Surgeon in Australia.
Apart from the general requirements, each surgical specialty has published criteria for how they will score and evaluate applications.
Potential applicants will take note of what items on their CV or application attract merit or attract points and will generally seek to maximise their total possible points.
Depending on the SET scheme points may be awarded for things like outstanding academic achievement in medical school, teaching and mentoring experience, research experience and/or completion of a higher degree, courses, surgical experience, and rural and remote experience.
In general, most applicants will “max out” their application score to the total amount possible for them.
This will often then make the referee reports more critical in determining who makes it through to interview.
Supporting Rural, Indigenous and Female Trainees.
RACS has developed a number of initiatives to support trainees from non-traditional surgical backgrounds, namely female trainees, trainees of rural backgrounds and Indigenous trainees.
In some instances, applicants may receive additional application points if they can demonstrate one or more of these backgrounds. Or there may be a set number of positions reserved for an applicant from any of these categories.
Referee Reports.
As mentioned referee reports are critical in the RACS SET selection process and the RACS takes the collection of references very seriously.
Given that the majority of applicants tend to “max out” their application score where they can, referee report scores tend to be more critical in determining who progresses to the interview as well as the overall outcome.
Get Help with your SET Interview Preparation
If you are appearing for the RACS SET Interview you can get some help and early assistance by attending our free webinar where Anthony takes you some of the tips and techniques he has used with past clients who have had success in their application.
The format of the interview is determined by each specialty group but is structured and in most cases conducted as a Semi-Structured or Multiple Mini Interview format. The distinction between the two is somewhat arbitrary as with semistructured there are usually 3 separate panels and with MMI around 6 panels. All questions have been carefully developed, scored and calibrated beforehand.
Interviews are usually given in a ratio of 3 interviewees to every one training post.
A number of “stations” are designed where candidates may be given questions based on clinical cases to discuss or provided with professional or ethical or other non-technical scenarios to work through.
SET Program
Application Fee
Application % Weight
Referees % Weight
Interview % Weight
Interview Format
Applicants 2020
Succesful 2020
Number of Attempts Allowed
Cardiothoracics
$840AUD
20%
20%
60%
Semi Structured
6*
Not Specified
General Surgery
$935AUD
35%
25%
40%
Semi Structured
323
108
Not Specified
Neurosurgery
$985AUD
10%**
30%**
30%**
Semi Structured
65
13
4
Orthopaedics
$840AUD
Candidates must meet a minimum CV score to progress to Referee Checks
25%
75%
MMI
219
54
4
OHNS
$900AUD
20%
40%
40%
MMI
97
15
4
Paediatric Surgery
$840AUD
Must achieve a minimum score on CV to progress
25%
75%
MMI
21
3
3
Plastic & Reconstructive Surgery
$886AUD
20%
35%
45%
Semi Structured
76
21
3 (4 with permission)
Urology
$840AUD
30%
30%
40%
MMI
51
21
3
Vascular Surgery
$840AUD
25%
35%
40%
MMI
42
9
3
* results for 2021 (Cardiothoracics did not select in 2020) **Neurosurgery also holds a neuroanatomy entrance examination worth 30%
Competition Rates.
As you can see from the above competition rates for SET training posts are fierce. For the year 2020 (if we ignore Cardiothoracics which did not appoint that year) we had 244 successful appointments amongst 894 applicants, which is around a 27% rate. According to the Neurosurgical Society of Australasia of 340 applicants across 6 years, only 63 appointments to training positions were made. Which is a less than 1 in 5 ratio.
3 Strikes and You Are Out
Bear in mind also that many programs will only allow you to apply a certain number of times. Normally a maximum of 3 times.
The Importance of Having a Plan B.
For all of the above reasons any doctor considering a career in surgery in Australia should definitely have a backup plan or alternative career path. Because even though you may be highly talented and knowledgeable about surgery it’s highly possible that there are even more talented candidates who rank above you.
Related Questions.
When does selection into RACS training occur?
Applying for and selection into RACS occurs very early in the year. Registrations usually open in January of each year and close in February. Applications usually open in February of each year and close in March. Application scoring, referee checking and testing then occur between March and April with interviews normally in June and offers announced in July.
What are the costs associated with applying for surgical training?
Applying for SET training is not cheap and the registration and application fee will normally set you back the best part of $1,700 AUD or more. Of course, there is also the cost of travel and accommodation to attend an interview and the cost of employing an interview coach to bear in mind.
Is there a typical surgical personality?
A number of scientific studies have examined the question as to whether there is a typical surgical personality that differentiates itself from other medical specialties for example this study demonstrated that surgeons are more extraverted and open to new experiences. Currently, RACS does not specifically select for certain personality traits. Although the use of an SJT could be seen as a proxy for this.
Given that doctors from Canada have the same preferred status in Australia as doctors from the United Kingdom, Ireland and the US. It’s really surprising that there are not more Canadian doctors in Australia. The same rules apply for Canadian doctors as per doctors from the above mentioned other countries. And employers are generally very open to an application from a doctor from Canada. Whether this is for a short-term working holiday or a permanent move.
So how can Canadian doctors work in Australia? The short answer is that if they are a trainee doctor they should apply for a vacant post under the competent authority pathway and if they are a recognised specialist in Canada they should first apply to the relevant college for recognition. Of course, no doctor coming from another country is absolutely guaranteed to be able to work in Australia. But if you are from Canada you have a very good chance.
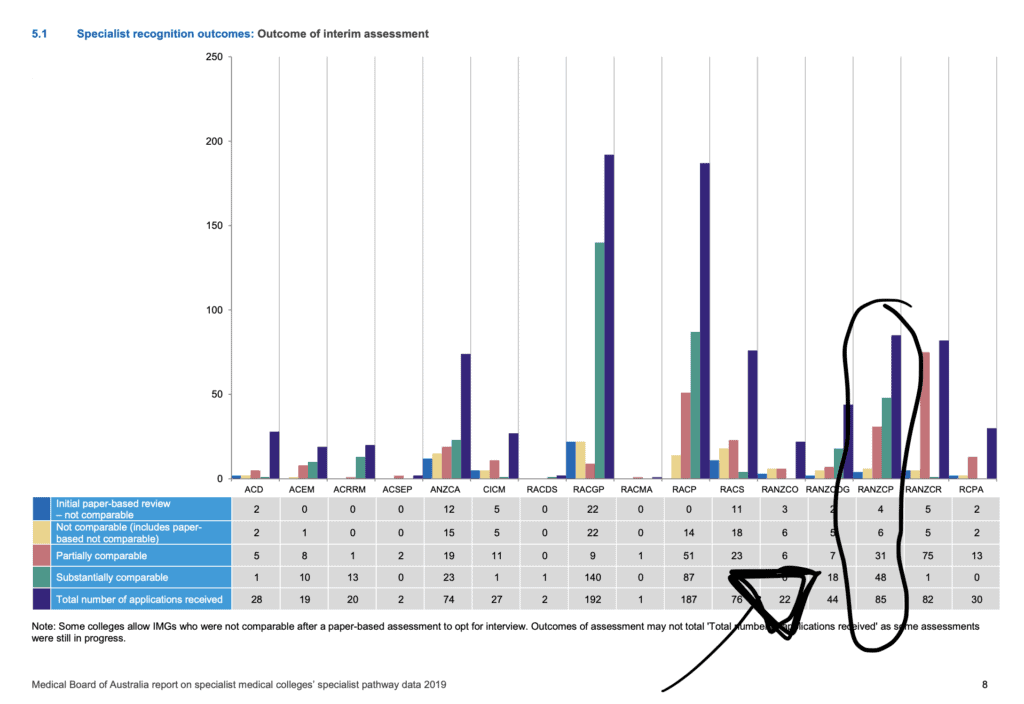
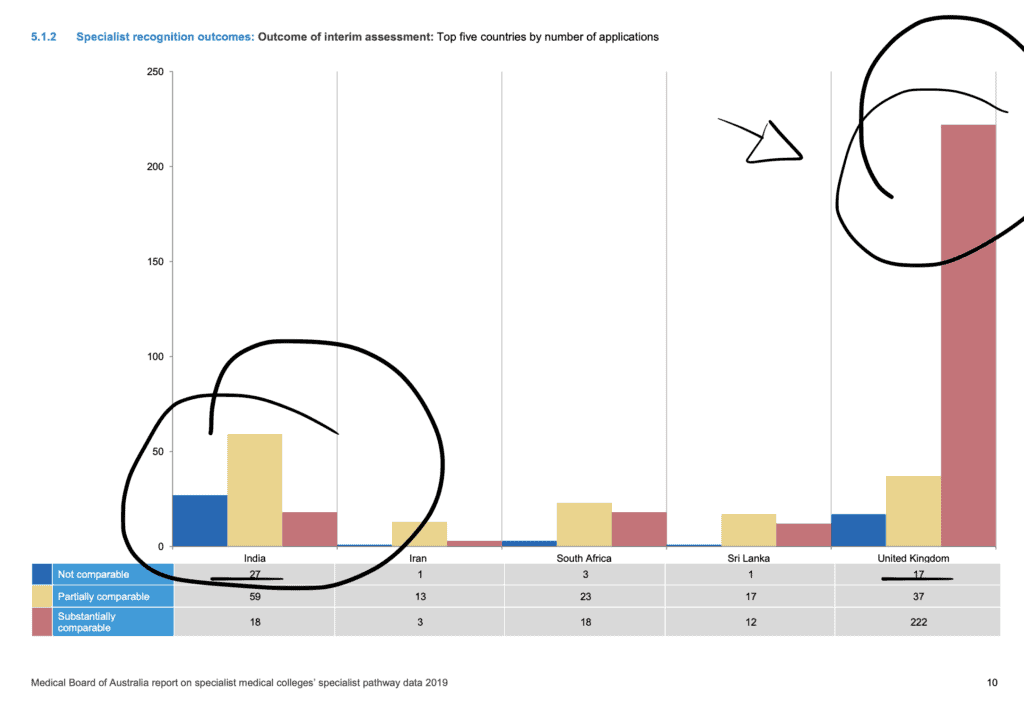
Because the Canadian medical training system is recognized by the Medical Board of Australia as being on par or what is termed “competent”, Canadian doctors have good success with either becoming generally registered through the competent authority pathway or being recognized as a specialist through the specialist pathway. In the year 2019 (the latest year we have figures for) 33 trainee doctors from Canada applied for registration in Australia with 31 of those applications granted. In addition, from the years 2015 to 2021, 94 Specialist doctors from Canada have applied for assessment in Australia with 82 being granted comparability.
So the prospects for Canadian doctors working in Australia are generally positive. But it’s important to have a bit more detail. As I have highlighted there are two main options for getting registered. So we will talk about these first and then go into some other common questions.
The Competent Authority Pathway. The Option For Trainee Canadian Doctors in Australia.
If you are a trainee doctor in Canada. Then you are most likely looking at the competent authority pathway for working in Australia.
The competent authority pathway assigns a preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States and the Republic of Ireland.
There is largely a historical rationale for this situation. It is based on the premise that all these jurisdictions have similar approaches to medical school training and similar standards.
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools, the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically to those from Australia. Or are more competent!
If you are an international medical graduate (IMGs) and you have achieved general registration in the United States, Canada or the United Kingdom (but not the Republic of Ireland) you are also eligible for the competent authority pathway.
So for doctors from Canada who did their primary medical degree elsewhere, this involves completing all steps of the Licentiate of the Medical Council of Canada and completing 12 months of postgraduate education or residency training in Canada, either as part of the LMCC or otherwise.
In essence, this is identical to the requirements that you would need to demonstrate if you had just graduated from a medical school in Canada.
What are the steps involved in the competent authority pathway?
What Types of Jobs Can I Apply for as a Canadian Trainee Doctor in Australia?
You can pretty much apply for any sort of trainee job. There are often a number of postgraduate year 2 or 3 general jobs on offer. They are normally termed Resident Medical Officers in most States and Territories, but may also be called House Officers or Hospital Medical Officers in some places.
Above these sorts of posts, come the specialty training positions. These are usually referred to as Registrar posts. Australia’s specialty training system is a little different to Canada’s in that Australian doctors do not immediately enter specialty training. You tend to enter specialty training around postgraduate year 3. You might also see advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most jobs you come across will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice, the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
your previous experience, especially in the type of position for which you have applied
whether you have practised recently and the scope of your recent practice
the requirements of the position including the type of skills required for the position
the position itself, including the level of risk, the location of the hospital or practice and the availability of supports (supervisors)
the seniority of the position, for a hospital position
In general, you will either be approved for Level 1 or Level 2 Supervision. If you are quite a senior trainee doctor in your own right you might be granted Level 3. There are 4 Levels and the higher up you go the less direct oversight you require.
Level 1 Supervision.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times and you must consult with them about all patients. Remote supervision (e.g. by telephone) is not permitted. This type of supervision is generally recommended when you are very junior yourself or entering a junior role with which you are not very familiar. In Australian major public hospitals, there are many layers of other doctors from who you can get supervision. So Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision.
Level 2 Supervision, which is what most competent authority trainees receive is a step up from Level 1 Supervision. Supervision must primarily be in person but your supervisor can leave you to do work on your own and you can discuss it by phone. You should discuss with them on a regular (daily) basis what you have been doing with patients. But do not need to discuss every case.
Level 3 Supervision.
Level 3 Supervision, is what you might receive if you are working in an Advanced Trainee role in Canada and transferring to something similar in Australia. In this case, you have much more primary responsibility for the patient. Your supervisor needs to make regular contact with you but can be working elsewhere and available by phone or video.
What happens after I commence my position?
Once you are approved for registration and you have your visa issues sorted you will be able to commence work. Generally, your employer helps you out with these things. You will be working under what is called “provisional registration” by the Medical Board of Australia.
Generally, all you need to do for these 12 months is to pay attention, show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia and it is your responsibility (not theirs’) to see that they are completed and returned on time. If all the reports go well you will be able to be recommended at the end of the 12 months for general registration.
You will probably be starting to look for another job or negotiating an extension around this time. With general registration, you may be able to apply for a skilled visa, as well as be looking at applying for permanent residency.
Permanent residency is crucial for applying for some specialty training programs. See below.
The Specialist Pathway. The Option For Canadian Specialists
For qualified specialists from Canada, your option for working in Australia is what is called the Specialist Pathway.
Actually, it’s a combination of the Specialist Pathway and the Competent Authority Pathway. More on that in a bit.
Once again your process starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need position, in which case the employer or recruitment agent will provide you with a lot of support and will likely pick up the costs of being assessed.
For most International Doctor specialists however these days you will be approaching the college directly to be assessed for specialist recognition. This is not something to be trifled with. The paperwork requirements and the cost (generally around $10,000 AUD or more) is considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
Specialist Pathway Course
Free Course
You can enrol now in this free course that will step you through all the requirements for working as a specialist doctor in Australia
We have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The majority of Canadian specialties (but not all) map to a similar college or specialty in Australia. So working out which specialty goes into which Australian college is generally not too confusing. We have put together a summary of the Australian specialist medical colleges here.
After you go through your specialist assessment you are given an outcome.
In the majority of cases for Canadian specialists, you will be deemed substantially comparable. This essentially means that you will need to work under some form of peer review for up to 12 months and so long as your reports are satisfactory you will be recommended for specialist registration at the end.
Occasionally specialists from Canada are deemed to be partially comparable (a situation where this may occur is if you have just recently finished specialty training but have not worked as a specialist for very long). In this situation, you will need to work under supervision for longer and may well also face some formal examinations.
Rarely are specialists from Canada deemed not to be comparable by the college. This has only happened to 12 out of 94 specialist doctors from Canada from 2015 to 2021. If you are deemed to be not comparable, this means you cannot directly become a specialist in Australia. You will probably have to go through the competent authority route and re-enter training in Australia.
Alternatively, if you are just looking for a short period of time in Australia you may want to consider the Short Term Training in a Medical Specialty Pathway.
How to Maximize Your Chances of Getting a Substantially Comparable Outcome.
To ensure that you are seen as substantially comparable by the relevant college I would recommend the following:
You should be recognised as a specialist in Canada and be a Fellow of the RCPSC or CFPC
You should ideally have worked substantively at a Consultant level in your field for 2 years or more
You should be able to demonstrate good standing with the Medical Council of Canada, your College and your employers
You should be able to demonstrate ongoing continuing professional development
You should prepare for your interview with the college as if it were an important job interview
Can you enter training in Australia if you are a doctor from Canada?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in many cases permanent residency or citizenship.
After receiving their general registration doctors from Canada can apply for specialty training in the same way that Australian trained doctors do. And if accepted will go through the exact training program and experience. Some colleges may offer recognition of prior learning for training you have done already. But this varies and may at best normally shave one or two years off from your training.
An Alternative But Limited Option.
There is an alternative but time-limited pathway for Canadian doctors who are just seeking a short-term experience in Australia to add to their training in Ireland. This is called Short-Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in Canada or be less than two years from completion. So this is a program mainly for early-career specialists or advanced trainees.
In this pathway, you go through the same steps with the AMC as per the competent authority pathway to gain registration. You will not, however, be able to apply for specialist assessment as part of this pathway. But if you gain general registration you may then be able to apply for another position and then apply for specialist assessment.
Generally Canadian doctors do not opt for this pathway as they have the option to get registered for these posts under the Competent Authority Pathway.
How many doctors from Canada are working in Australia?
There is no one public data source to tell us how many Canadian doctors are currently working in Australia.
From data collected by the Australian Government, we know that for 2018 and 2019 (the latest available years):
In 2018, 21 applications were made for registration under the Competent Authority Pathway with 20 being granted.
In 2019, 33 applications were made for registration under the Competent Authority Pathway with 31 being granted.
So the best estimate is that there are probably a few hundred Canadian doctors working in Australia.
It should also be noted that quite a few students come from Canada to Australia to study medicine.
Costs of Moving To Australia and Working As a Doctor.
There are lots of costs to consider when thinking about moving to Australia to work as a doctor.
There are some direct costs to consider. Most of which relate to the bureaucratic process of being assessed and gaining registration.
Some of the costs you may be up for, include:
AUD (unless otherwise noted)
Establish a Portfolio with the Australian Medical Council
$600
Registering with EPIC and having one primary degree checked
$125 USD + $80 USD
Medical Board Application Fee for Provisional Registration
$430
Medical Board Application Fee for Specialist or General Registration
$860
College Specialist Assessment Fees
$6,000-$11,000
College Placement Fees (for the period of supervision)
$8,000-$24,000
Costs for Working as a Doctor in Australia
Further, if you are required to undertake further exams there will be a cost for this as well. As an example, RACS charges an exam fee of $8,495.
The Cost of Your Time and Effort.
For all of this financial cost, you will also need to factor in the cost of your own time. It takes a lot of effort and persistence to deal with the paperwork and track down the records you need.
In addition, you are probably going to have to pay costs in your own country for things like records of schooling and certificates of good standing.
There are also visa costs.
And then there is the cost of airfares and transporting your belongings halfway across the world.
Depending on where you work in Australia you may find that the cost of living is higher or lower than you are used to. House prices and therefore house rental rates have gone through the roof in Australia in the last decade or so but are starting to come down.
You will probably have to factor in some initial extra hotel or short term rental charges whilst settling in and you may find if you have children that you have to pay to enroll them in school as public schooling is only generally free if you are a citizen or permanent resident.
If you are lucky and in one of the specialty areas of demand your employer may offer to pay for some of these costs. Its certainly worth asking about it.
We hope that you found this summary about how Canadian doctors can work in Australia useful. If you have any questions or queries or just want to relate your experience. Please feel free to leave a comment below. We would love to hear from Canadian doctors who have made the journey to Australia.
Get a Clarity Call
If you are wanting to gain further guidance about your personal situation or just get some answers to questions then you can book a RISK-FREE Clarity Call. Held over Zoom
Answer. Doctors from Canada are amongst a select group of countries for which the Medical Board does not expect an English proficiency test. However, there may still be some circumstances where you do need this. If, for example, some of your schooling was in another country. You should always check the requirements.
Are there any other options for working as a Canadian doctor in Australia?
Answer. Some doctors just want to come to Australia for a limited period of time as an opportunity to train in another country. As we have highlighted above there is an alternative but time-limited pathway for Canadian doctors who are just seeking a short-term experience in Australia to add to their training in Canada. This is called the Short-Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in Canada or be less than two years from completion. So this is a program mainly for early-career specialists or advanced trainees. Most Canadian doctors do not use this pathway as the Competent Authority Pathway is more accessible and able to be used for the same purpose.
Should I use a medical recruitment company if I am considering working in Australia?
Answer. It is possible to deal directly with employers in Australia. In general, however, when moving from one country to another most doctors find it useful to engage with a medical recruitment company as they can tend to take some of the stress out of the planning for you and help with all the paperwork and negotiating with prospective employers. Some medical recruitment companies also provide migration services and relocation services as well. We have written more on this subject here. And a list of medical recruitment companies is available here. Feel free to contact us first for recommendations.
How hard is it to become a specialist in Australia if you are from Canada?
Answer. Specialist doctors from Canada are not automatically granted specialist recognition. However, most are. Canada has generally one of the highest rates for doctors being seen as substantially comparable.
Are there any particular specialties that are easier to apply for?
Answer. The majority of specialties have some vacancies and will provide opportunities for Irish and other IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be quite difficult. On the other end of the spectrum general practice, psychiatry and most parts of critical care medicine are often always looking for doctors.
Doctors are often put into positions that can cause them stress, burnout and depression. Many doctors will reach a stage in their career when they question their choice to practice medicine. If this sounds like you then perhaps the concept of Ikigai is worth reflecting upon. Ikigai is a Japanese word that roughly translates to “reason for being.” It is similar to the French term raison d’etre.
If you are able to combine Ikigai and Medicine. It could be the reason why you get out of bed in the morning. Ikigai can be found through any activity that brings joy, which is why it’s important to find these activities and indulge in them more often. The problem is there are powerful barriers in Medicine that can prevent us from finding our Ikigai. Most notably salary expectations and the stigma of being seen to “reject” a career in medicine for something else.
Venn diagram exploring the Ikigai concept. Note this is based on the Western author Hector Garcia’s conceptualisation of the idea and not a true representation of the original concept.
The Japanese Concept of Ikigai
Ikigai is closely tied to the Japanese concept of Seika (貞知). Seika is about making the most of your life. Every human being has the opportunity to lead a fulfilled and happy life. The concept of Ikigai, which was formed by Japanese author Haruki Murakami. Ikigai does not require that an individual’s pursuit of happiness be grandiose or complicated, nor does living a fulfilling life mean achieving success as defined by society; one might find meaning in their work as an engineer for example.
Everybody has a reason for living. For many of us, pursuing our goals and passions is sufficient motivation to meet life’s challenges. But some people have trouble identifying what is important to them. Sometimes it takes a tragedy or a crisis to help with this realization, but most often, it just happens naturally as we grow older.
Moral Injury and Medicine
Working in the medical profession, we can often encounter a stage where we question our worth or whether it is worth it. We may feel guilty or ashamed of what we are doing in our work. It is a very common feeling and one that can be extremely debilitating. One reason we may question our worth as medical professionals is through moral transgressions.
Most of us are taught early on that the right thing to do is the moral thing to do. It means that you are doing what is right. If you are forced into a position of not doing exactly the right thing. You might think that it is not very important, but it still matters because if you do things differently, then you are doing something wrong by being bad. If you are constantly put in a position where you feel you are not doing right, it will eventually challenge your resilience and cause moral injury.
Moral injury is a concept in psychology and psychiatry. It is thought to arise from feelings of guilt or shame felt by an individual who has taken part in wrongdoing, for example, war crimes, genocide, torture, or other such atrocities. Whilst these are extreme examples of wrongdoing we can also experience moral injury if we are constantly put in a position in our work of feeling that we are not doing good or constantly having to compromise on what is right.
A classic example in medicine might be the feeling that we are constantly medicalising people’s problems, i.e. providing medications or physical treatments when the root causes are far deeper than this. Or being forced to discharge patients when the care available at home is inadequate because we need to create beds for “sicker patients”.
Finding Your Ikigai in Medicine
As I have noted, Ikigai is often translated as ‘reason for being, the reason why you get up in the morning. It is believed that your Ikigai must be fulfilled before you can die. While it is not always easy to find one’s Ikigai, there are some things to remember when searching for it.
How to find your Ikigai
Many people search for a sense of meaning or Ikigai in their life. You may find your Ikigai by doing what you love and pursuing your passions. Ikigai is found through actions and not just through words. It can be found in medicine, as well as other professions. For those of us looking for our Ikigai, we can find it most easily by taking action and finding the things that speak to us and energize us.
It is important to understand that Ikigai is not just about your own personal purpose and fulfilment. It is also about your contribution to society at large. In the end, Ikigai should bring meaning and purpose to your life while you contribute to the good of others.
It is said that everyone has an Ikigai – their particular intersection of passion, talent, and potential to benefit others. It is only a matter of finding it. The journey to Ikigai, however, might require significant time, reflection, and effort to get there.
From a personal perspective. As someone who has always felt a little edgy about their career and a desire to try new things. I wonder if Ikigai is perhaps more of an iterative process for some.
But How Does Ikigai Pay the Bills?
Ikigai is not just about finding meaning and purpose. It can also be about making money.
Ikigai can be a way to work out how to make a living whilst feeling fulfilled and with purpose. Ikigai does not have to be part of your formal career. It can be part of your hobbies, your family or a profession. Ikigai is not necessarily tied to a job, but it is tied to a passion. It is about finding the job that is the right fit for your passion.
In order to arrive at our Ikigai, we can consider four key spheres. (Note: this concept relates to the author Hector Garcia’s conceptualisation of Ikigai, not the original Japanese concept)
I Love It!
Clearly, this sphere encompasses what we do or experience that brings us the most joy in life and makes us feel most alive and fulfilled. This might be playing cricket, singing in a bad, playing computer games, hanging out with friends or travelling the world.
What is important here is to think about what we truly love without thinking about whether we are good at it or not and whether we can earn a living from it. This is the most indulgent sphere.
Something I Am Great At
This sphere includes anything you are particularly good at. These can be skills you have learnt or hobbies you have pursued, or talents you have had from an early age. What you are good at might be, for example, playing the guitar, displaying empathy, sports, performing surgery, or painting pictures.
This sphere encompasses talents or capabilities, whether or not you are passionate about them, whether the world needs them, or if you can get paid for them.
The World Needs This
Whether it’s the entire world or a small community you are in touch with. The “world’s” needs might include skilled doctors, clean energy, volunteers, or improved teacher training.
This is the area of Ikigai that is most practical. It connects most explicitly with other people and doing good for them beyond your own needs.
Can I Get Paid For This?
This dimension of the Ikigai diagram also refers to the world or society at large. It involves a transaction where someone else is willing to pay you for something you provide. Or that there is a market for your skills or expertise. You might be passionate about your poetry writing or be very good at canoeing, but this does not necessarily mean that you can get paid for it.
Whether you can get paid for your passions or talents depends on factors such as the state of the economy and whether your passions or talents are in demand.
Ikigai and Medicine – Threading the Needle?
What I notice most about the Ikigai concept is how much overlap one needs between these 4 spheres of love, good at, need, and monetizable.
I suspect it is for this reason that many of us settle on compromises where we end up doing things that the world needs (and there are plenty of medical jobs that fit this bill) or things we are good at. So we can get paid for our efforts. But missing any passion or sense of mission for what we are doing.
Barriers to Ikigai in Medicine
You only have to work your way through this recent post to see that money is probably one of the biggest barriers to doctors gaining a sense of purpose and Ikigai.
If we are lucky, we do find an area of medicine we truly love. That has a need and needs us and our skills. But it may well mean that we compromise on our salary expectations somewhat. I say somewhat because a salary compromise in a medical career still represents an outstanding salary in most other people’s careers.
So, for example, even though we are quite good at surgery. We might choose to work in general practice as we have more autonomy over our patient care decisions and get to work holistically with people which we love. In so doing, we probably compromise somewhat on salary expectations. But we probably also create room for other things we love in life, like family and hobbies.
However, as doctors, we have the potential to create economic expectations for ourselves that can trap us in careers that are creating us harm. Doctors generally have good credit risks. So we often end up servicing high loads of debts and other financial expectations, which can make exciting a particular medical career difficult.
Finding Your Ikigai Alongside Medicine
Perhaps your medical job is not your be-all and end-all. Perhaps it’s your way of paying for the thing in life that brings you passion and satisfaction and others enjoyment?
I certainly know of many doctors who work so that they can indulge their passion in music or the arts and, in so doing, bring joy and something to others that they need.
Consider also those doctors who do stints working for organisations like Doctors Without Borders. The years of critical care training and experience at home may not be exactly what they would like to be doing on a daily basis. But the trips abroad where they can “make a real difference” helped to balance out having to fight the bureaucracy of hospital care in your real job whilst you are maintaining and improving upon your skills.
Finding Your Ikigai Out of Medicine
And finally. Maybe it’s just possible that the skills, talents and passions that brought you into Medicine are the sorts of skills, talents and passions that are needed in other parts of our world.
Maybe. Just maybe. It’s possible for you to find a career completely outside of medicine.
Here is where I think doctors face another real but under-recognised barrier to finding their Ikigai. Which is the stigma and possible shame or guilt associated with being a doctor who is no longer a doctor.
I was once providing career coaching for a doctor who was considering exiting medicine altogether for a career in real estate.
Real Estate happened to be something that she loved and was very good at. Having flipped several properties on the side during her medical school and training. And, of course. The world needs houses.
What surprised me most of all about our encounter was her statement that I was the first doctor that she had ever talked to who would even consider not working in medicine as a possible career choice.
A couple of years ago I wrote this post reflecting the fact that according to the Australian Taxation office doctors are extremely well paid in Australia. This blog is both an update to that post. But also a focus on who are the highest paid doctors in Australia? This time I am going to try to go into more detail as I had lots of questions last time, likes “what about pathologists?” or “I’m a neurosurgeon is that any different from an orthopaedic surgeon.
First for the overview:
Just like 2 years ago if we look at things at a macro level not much has changed and doctors still maintain their high rankings in the ATO data, with Surgeons sitting at number 1 on an average taxable income of $394,303 AUD. Followed by Anaesthetists at number 2 on $386,065 AUD, Internal Medicine Specialists at number 3 on $304,752 AUD and Psychiatrists ($235,558 AUD) and Other Medical Specialists ($222,933 AUD) at 5th and 6th. Just squeezed out for number 4 by Financial Dealers. This is in fact the same as it was 2 years ago.
But if we go down to a more granular level and look at subclassifications where Surgeons are divided into specialties like Neurosurgery and Orthopaedics and Internal Medicine Specialists are divided into specialties like Cardiology and Paediatrics we see that some medical specialists do even better with medical professionals dominating 34 of the top 50 occupations for average taxable income in Australia.
With the highest paid occupations and the highest-paid doctors being Neurosurgeons coming number 1 at $575,687 AUD, followed by Ophthalmologists at 2 with $524,804 AUD and Ear Nose and Throat Surgeons 3 at $468,525 AUD. What is also interesting is the huge discrepancy in earnings between male and female doctors of all specialties with a male Neurosurgeon earning more than double the average taxable income of a female Neurosurgeon $629967 AUD vs $304,290 AUD.
Read on further for some further analysis and discussion about medical specialist salary in Australia.
Australia’s Highest Paid Doctors Still Do Very Well in Comparison to Other Occupation Groups
Here’s a list of the top ten occupation groups by Average Taxable Income for 2018 to 2019 (the most up to date figures).
[ninja_tables id=”126355″]
Surgeons sit at number 1 on the list on an average taxable income of $394,303 AUD. Followed by Anaesthetists at number 2 on $386,065 AUD, Internal Medicine Specialists at number 3 on $304,752 AUD and Psychiatrists ($235,558 AUD) and Other Medical Specialists ($222,933 AUD) at 5th and 6th. Just squeezed out for number 4 by Financial Dealers. This is in fact the same as it was 2 years ago.
In fact, according to the ATO Surgeons have been topping the list (for occupation groups) since 2010.
Now some of you with a keen eye will have noticed that if we look at the fifth and final column would have noticed that if we go on median taxable income then it is actually the Surgeons colleagues the Anaesthetists who are the better paid. What’s all that about then?
Well, first we have to understand what is meant by taxable income.
According to the ATO: Your taxable income is “the income you have to pay tax on” (d’oh!).
More precisely.
The taxable amount is the amount left after you claim a deduction for all the expenses you can. These amounts reduce the amount of assessable income you pay tax on.
Assessable income − allowable deductions = taxable income
So we have average taxable income and median taxable income. If we recall our statistics from high school average generally refers to the mean.
We calculate the mean by adding up all the values (in this case taxable incomes of Surgeons) and divide the sum by the total number of values (the number of Surgeons who completed a tax return). The median is calculated by listing all numbers (taxable incomes) in ascending order and then locating the number in the centre of that distribution.
Now. I’m only speculating here. But the most likely answer to why the big difference is variance.
And this is borne out when you look at some of the more detailed tables below.
Whilst the ATO doesn’t help us out with confidence intervals or ranges. It’s most likely that the statistics for Surgeons are more skewed by a small but significant group of Surgeons doing particularly well as some of the highest paid doctors in the country.
Another way to look at it is. Working in Anaesthetics you can make some really good but steady income. But you are probably less likely to be declaring $1million per annum. Whereas as a Surgeon you are more likely to have that opportunity.
And of course, we need to also account for the fact that the ATO does not collect statistics on hours of work. It’s a safe bet that many doctors are doing more than 40 hours a week. But there will be a number who will also be working part-time. We know that different occupations in medicine tend to have different percentages of doctors who work full time versus part-time. So this will have some impact as well.
For example in a fairly recent Australian Institute of Health and Welfare Report average weekly hours worked across 20 specialties varied from 38.2 hours per week (Psychiatrists) to 54.1 hours per week (Intensive Care Physicians).
When We Look Even Further Australian Doctors Are Almost Universally Well Paid
As I said the last time I blogged about these statistics I had lots of questions about different scenarios. Like what if I am this particular type of Surgeon? Or you haven’t talked about Pathologists. Or what about if I work privately versus publicly.
So let me attempt to address as many of your questions as possible in the next 3 tables.
Firstly below I have listed the top 51 occupations by taxable income in Australia for 2018 to 2019 again according to the ATO. Why 51? Well. If you go through this table you will see that 32 of the 51 occupations here are medical practitioner occupations.
So medical practitioners also occupy 32 of the top 51 occupations in Australia.
[ninja_tables id=”126336″]
Now. What you might be surprised to know is this. There are only 2 other medical occupations that are not on this list. Which are 253000 Doctor – Specialist – type not specified, which sits at 217 at $137,480 Average Taxable Income and 253112 Medical Officer – Resident which sits at 422 on the list at $107,191 Average Taxable Income. And arguably these are the two categories that will cover most trainee doctors.
The list is of occupations is 3535 long by the way. So even if you are a Medical Officer – Resident you are already sitting in the top 12%.
And if you are a specialist you are doing very well in comparison to most other occupations.
So if you have a particular thesis that a certain occupation in medicine is poorly done by. Then I’m sorry to burst your bubble. But the data doesn’t support you. At least if you are comparing doctors to the rest of Australia.
Another way of putting it would be that the highest paid doctors in Australia are doctors. But clearly to paraphrase George Orwell. Some doctors are more highest paid doctors than other doctors.
The Highest of the Highest Paid Doctors in Australia Are Proceduralists
Have a look at the top of the table. Neurosurgeons have the highest average taxable income in Australia at $575,687 AUD. Then come Ophthalmologists, ENT Surgeons, Cardiologists, Urologists, Orthopaedic Surgeons, Plastic Surgeons, Vascular Surgeons and Gastroenterologists.
It’s only at number ten that a non-medical practitioner occupation makes an appearance. And that’s Judges!
What do the top nine all have in common? They perform procedures. There is a common conception that if your medical specialty includes significant procedural work (for which you can bill) you will do better from a monetary perspective. And here is some evidence that supports that idea, i.e. the highest paid doctors are procedural doctors.
If we go down the list further. The next 6 specialists are also involved in procedures. It is not till we hit Medical Oncologist on the list at 17 that we encounter a medical specialist who arguably does not have the opportunity to perform a lot of procedures.
Oh. And then we hit our next non-doctor at 18. The Financial Investment Manager.
I am often asked by international medical graduates which specialties are hard to get into in Australia. With the exception of Radiologists and perhaps Oncologists. This list of the top 18 highest paid doctors is a good reference of specialties where you are more likely to struggle.
Another 6 medical occupations (total of 24) come before State Governors at 28 on the list of highest paid occupations. (I’m also wondering how there are 23 returns for State Governors, given there are only 6 States, 2 Territories and one Commonwealth?)
General Physicians make on average slightly more than Magistrates and Psychiatrists are only just beaten by Members of Parliament. There are only 3 medical occupations that make less on average than Dentists and Cricketers.
Surprisingly, General Practitioner is not last on the list of Medical Practitioners. Its Pathologist.
Which Doctor Occupation Am I In?
Now you may be wondering what is covered by these doctor groups. As I said I got lots of questions about this last time.
To understand the way the ATO classifies occupations we need to refer to the ANZSCO classification system.
The Australian and New Zealand Standard Classification of Occupations (2013 version 1.3) is a joint collaboration between the Australian Bureau of Statistics (ABS) and its New Zealand counterpart, StatsNZ.
According to the ABS:
ANZSCO provides a basis for the standardised collection, analysis and dissemination of occupation data for Australia and New Zealand. The use of ANZSCO has resulted in improved comparability of occupation statistics produced by the two countries.
ANZSCO has a 5 level hierarchy starting with Major Groups, Sub-Major Groups, Minor Groups, Unit Groups and finally Occupations.
So when the media claims that Surgeons are the highest-paid occupation in Australia they are technically not correct. They should be referring to Neurosurgeons (see below).
There are 8 Major Groups
Managers
Professionals
Technicians and Trade Workers
Community and Personal Service Workers
Clerical and Administrative Workers
Sales Workers
Machinery Operators and Drivers
Labourers
With the notable exception of perhaps medical administrators (who perhaps are technically classified under Managers), all other medical practitioners are classified under Professionals > Health Professionals > Medical Practitioners.
I also suspect however that Directors of Medical Services and the like do not classify themselves as Medical Administrators as the average taxable income of $55,000 really does not make sense for this occupation. So I suspect they are selecting another medical occupation when completing their tax return.
This brings me to an important point. The ATO doesn’t audit (as far as I know) what occupation you put down on your tax return. So there is an element of discretion here.
On this point. It’s possible that some university academic doctors also elect to classify themselves as Educational Professionals > Tertiary Education Teachers > University Lecturers and Tutors.
But returning to our classification of Professionals > Health Professionals > Medical Practitioners. Medical Practitioners is the Minor Sub Group.
The Occupational Groups below this Minor Sub Group with their Occupation Sub Set are:
Occupation Group
Occupations
Other Titles or Specialisations
2531 General Practitioners and Resident Medical Officers
253111 General Practitioner 253112 Resident Medical Officer
General Medical Practitioner Medical Intern
2532 Anaesthetists
253211 Anaesthetist
Intensive Care Anaesthetist Obstetric Anaesthetist Pain Management Specialist
2533 Specialist Physicians
253311 Specialist Physician (General Medicine) 253312 Cardiologist 253313 Clinical Haematologist 253314 Medical Oncologist 253315 Endocrinologist 253316 Gastroenterologist 253317 Intensive Care Specialist 253318 Neurologist 253321 Paediatrician 253322 Renal Medicine Specialist 253323 Rheumatologist 253324 Thoracic Medicine Specialist 253399 Specialist Physicians nec*
Intensive Care Medicine Specialist & Intensivist are alternative for Intensive Care Specialist
The only specialisation options for paediatrician are Neonatologist and Paediatric Thoracic Physician
Occupations in the nec group include: Clinical Allergist Clinical Geneticist Clinical Immunologist Clinical Pharmacologist Geriatrician Infectious Diseases Physician Musculoskeletal Physician (NZ) Occupational Medicine Physician Palliative Medicine Physician Public Health Physician Rehabilitation Medicine Physician Sexual Health Physician Sleep Medicine Physician
2534 Psychiatrists
253411 Psychiatrist
Specialisations: Adolescent Psychiatrist Child and Adolescent Psychiatrist Child Psychiatrist Forensic Psychiatrist Geriatric Psychiatrist Medical Psychotherapist
Alternative Titles for Otorhinolaryngologist are Ear, Nose and Throat Specialist Head and Neck Surgeon
2539 Other Medical Practitioners
253911 Dermatologist 253912 Emergency Medicine Specialist 253913 Obstetrician and Gynaecologist 253914 Ophthalmologist 253915 Pathologist 253917 Diagnostic and Interventional Radiologist 253918 Radiation Oncologist 253999 Medical Practitioners nec
Specialisations for Pathologists are: Clinical Cytopathologist Forensic Pathologist Immunologist
Occupations under Medical Practitioner nec are: Nuclear Medicine Physician Sports Physician
c/- Australian Bureau of Statistics
*nec = not elsewhere classified
In any case, you can now go look up the code that best represents your specialty and get some more detailed information of your earning potential from either the table above or the next one below. I’d recommend the next one.
And if you still can’t find yourself on the list. Feel free to have a wander through the ANZSCO information yourself.
The Highest Paid Doctors in Australia Are Men
You may not be all that shocked to know that male doctors do better than their counterparts.
What shocked me however was the extent to which this occurs. Try clicking on ‘M’ and ‘F’ and leaving ‘Total’ off on the table below.
[ninja_tables id=”126342″]
You see a wall of blue.
Click on the pagination tabs to see some pink.
If we filter for M & F and Neurosurgeon we get the following result:
What’s most curious to note here is that the 30 female Neurosurgeons almost match their 150 male colleagues in terms of average wage income. This would indicate to me that they are earning similar salaries from public health service roles. In fact, the median salary or wage result tends to indicate to me that proportionately female Neurosurgeons might be working more in the public health system than their male counterparts. It’s clearly non-salary or wage income that is making the difference here.
This will undoubtedly be partly related to other income through operating a private service. But is probably also due to income from other sources such as investments.
This leads to the following result. In the top paid occupation in Australia, men more than double the average taxable income of women.
And it’s the same result for each specialty. There’s not one specialist occupation in Medicine where women do better than men in terms of average taxable income.
How Does this Income Compare to Salary Information?
Most general practitioner specialists and trainees work in the private sector in Australia. As do a significant number of other specialists. So the ATO data will reflect that many doctors are working for themselves on a fee for service or contractual basis. If a doctor wants to earn a more regular income or salaried wage then they will generally opt to find employment in the public hospital system as a Staff Specialist.
As a point of reference to the ATO data, a full-time employed Staff Specialist in the NSW Health system will generally be earning between $246059 and $303643 depending on their year’s of experience and level of seniority. Although they may earn as much as $484799 if they opt to split their private billings with the health service.
So whilst you clearly need to be doing some private practice to hit the top of the income tables. You can see that for most specialties you can actually do better than the average amongst your peers by working in public.
In a future post, I will update you on the salaried rates of pays for trainee doctors.
Each year I do a round 700 hours of coaching with various clients for job interviews. Clients often ask for advice on what to do if they make a mistake in a job interview? What should you do if you make an error or stuff up? There’s quite a few posts about what you should do after a job interview if you realize you have made an error. But not so many about what you can do to effectively recover from a mistake in a job interview.
Some quick tips for dealing with making a mistake in a job interview include: taking your research notes about the job with you to the interview to help you, apologizing as soon as possible if you make a mistake, and asking for clarification or taking a sip of water if you are having a mental block. A half answer is better than no answer at all. And always leave the interview on a positive by thanking them for their time, even if you feel you have performed poorly.
Let’s go through some of the various scenarios now in more detail.
How to Prevent Yourself From Making a Mistake in a Job Interview
Before I discuss how you can recover from your mistake in an interview. Let’s talk about how you can prepare yourself effectively so that you minimize the risk of an error.
The most obvious thing that you can do to prevent yourself from making a mistake is to give yourself plenty of time to research the role and practice possible interview questions.
But what if you don’t have a lot of time to prepare and practice?
My favourite strategy for getting ready for a job interview will also help you to be better prepared for questions. With the bonus of something handy to take with you into the interview.
I call this process job alignment.
Put simply draw up a table with 3 columns in it.
Column A will be the selection criteria. Put each criterion in a single row by itself. And if there are other topics in the job description that you think might be relevant to the interview questions, for example organizational values. Put these in a row as well.
Column B is your evidence. You have probably already considered this in your application. But put it down again and go over it thoroughly. Do you really meet the criteria? Can you explain this effectively. Does your evidence include examples of achievements and outcomes?
Your final Column is Column C. And it is here that you want to come up with at least one good example that shows how you meet each criteria.
With this job now done you are armed with the information, you need to succeed in your interview.
What to do if You Make An Error in Your Answer?
Okay you have made it to your job interview and you have prepared your best. But sometimes things just happen.
So what should you do if you realize that you have made an awful mistake in answer to one of the questions posed?
Recover Quickly if You Can
If you realize mid-answer that you have made a fundamental error. For example, maybe you got the dosing of a medication wrong. It’s best to apologize straight away and correct your mistake. Then move on.
Whilst making mistakes in a medical job interview can be particularly fatal. Correcting yourself may actually be seen as a good sign. After all, errors do occur in medicine and if you can recognise one in yourself then you are showing a good trait.
Don’t Disrupt the Interview Flow to Correct a Mistake in a Job Interview
One thing you don’t want to do is disrupt the interview flow in order to correct a mistake.
If you do realize halfway through the interview that you made a mistake in question 1. Make a note. Write yourself a quick bullet point if you can.
Then when it comes time for the wrap up of the interview. Take the opportunity to add a correction.
Don’t make a big deal of your error. Just quickly point out that you want to correct something you said earlier and state your correction.
What to do if You Have a Mental Block?
We have all been there. You get asked a question that you know that you have prepared really well for. But your mind turns to fog. Perhaps you struggle to remember a term or a diagnosis or a name of someone important that you want to mention.
The first thing to do is to avoid panicking. Ask the interviewer if they can repeat the question. You can use this time to think. There is also nothing wrong with asking for a few moments or taking a sip of water. If you are still struggling after all this, then you should at least deliver a half answer as this is better than no answer at all.
Again. Some additional information may come to you by the time the interview comes to a close. If so request to add some clarification to your interview.
What to Do if You Are Asked an Odd or Confusing Question?
If you have done your preparation effectively you should be able to anticipate the intent of each interview question. But occasionally interview panels design weird questions for which the reasons are not immediately obvious. Sometimes these questions are designed to determine whether you have the skills or attitudes required to complete the job you are applying for.
If you are confused by a question or the angle in which you should respond, always try to bring your answer back to demonstrating a skill or quality you possess that shows you are able to do the job. This is a great time to consult your job alignment table for some inspiration.
Again. You may want to ask the interviewer for clarification or to put the question in a different way.
Make an Apology. But Don’t Over Do It
If you make a mistake during an interview, a simple apology can quickly remedy the situation. But don’t let this linger. Try to turn the interview back to a positive.
Focus on What You Bring to the Role
Once you have apologized focusing on your professionalism and qualifications can help save your application. For example, if you make an error discussing a clinical scenario. Try to point out how you are very systematic in your clinical practice and all the things you have learnt to do to remove errors from your practice.
Thank Them for Their Time
Even if you feel you have made a really bad mistake in a job interview be sure to end the conversation on a positive. The best way to do this is by telling them how thankful you are for their time and attention. This could potentially balance out your mistakes.
Use This Experience to be Fully Prepared for the Next Interview.
If you make a mistake in a job interview. Learn from your mistakes to present the best version of yourself in the next interview. For example, if you realize you were thrown by a number of the questions asked during your interview, write as many of them down as you can remember. And practice these questions for next time.
Forgive Yourself for Making a Mistake
Try to use your mistakes as a learning experience to make future interview performances more impressive. And most importantly, forgive yourself, because mistakes do happen.
*We will be regularly updating this post as the various States and Territories update their processes. Where information is not currently available for the 2021 year we have used information from the previous year, i.e. 2020.
It’s that time of the year again, where the whole medical internship Australia system kicks into gear. The time when each of the States and Territories in Australia open up their process to allow applications for medical internships for the following year. For four years I was responsible for running the largest Intern application system in Australia for 4 years. The NSW Intern application system. So I’d like to share with this year’s medical graduates some of the wisdom I gained from that experience.
(Disclaimer: all information here has been sourced in good faith but things do change so you should always do your own due diligence in such matters, we are providing this information to aid you in your application but take no responsibility for any outcomes)
As has been the case in past years the main Intern application and allocation dates are aligned across Australia so that every State and Territory opens and closes their systems at the same time and makes offers at the same times. There are some variations to this in relation to special priority categories in some States and Territories. The key things that all medical graduates should consider in preparing their medical internship application for the 2022 year in 2021 are as follows:
Applications open on 4th May 2021.
Applications close on 3rd June 2021.
Make sure that you have an Intern Placement Number otherwise you won’t be able to apply.
You should research the application requirements now as there may be some “surprises”. As soon as the application system opens, register or log in and ensure that you have everything you need to complete your application.
Understand where you sit in the priority list for any State or Territory you are applying to.
If you are required to attend an interview. Make sure that you have obtained leave from your medical school requirements to attend.
Also, consider that the interview is likely to be either via phone or video this year.
Give yourself time to request referees, put together a Resume, if required and find other documents that you may need.
The first main round offers come out from 12th July. So make sure that you have regular access to your email as your time for accepting offers can be quite short.
Stay in touch with your medical school. you may be worried about completing your degree on time but they are all working very hard with the other institutions to give you the best chance of completion.
Tip #1. Your Medical Intern Placement Number.
The IPN is a unique nine-digit number that has been generated by AHPRA and has been provided to medical schools for distribution to all 2021 final-year medical students. The number is used as part of the national audit process (which ensures that intern positions across the country are made available to as many applicants as possible) as well as to streamline registration.
This number is not the same number as your AHPRA registration number or student number. If you have not received you IPN you should check with your school.
If you are not an Australian medical student you won’t be issued an IPN. If you are applying as a non-Australian medical student you do not require an IPN. However, please note that unless you are a New Zealand medical student your chances of gaining an internship are very slim.
Tip #2. Other Things You Will Likely Need.
The majority of States and Territories require you to upload an academic transcript as proof that you are indeed a medical student.
They will also request evidence that you satisfactorily meet the AHPRA English Language requirements. This may seem a bit ridiculous given that you have been attending medical school in English for the last 4 or 5 years. But it is the law. So check whether you may need to submit an up-to-date English test result or some other form of documentary evidence such as a high school certificate.
Some States and Territories have a CV template that they suggest that you use to fill in your information. In the case of Victoria, you are required to use this template. It’s probably fairly harmless to use the template for the other States and Territories. But if you are thinking about your future career, then nows is a good time to be designing your own CV. The risk of using the template is that you don’t stand out from other candidates.
You will need to also provide proof of your identity, citizenship, residency, or visa. And if you have had a name change along the way you will probably also need to provide some documentation in relation to this.
Why All This Information?
The State and Territory bodies who administer the Intern application process have a responsibility to ensure that you are eligible to apply for provisional registration at the end of the year in order to work as an Intern. They collect this information to check that everything is in order so that you are indeed eligible to apply. Employers can get rightly annoyed when told that someone who has been allocated to work with them as an Intern will have a several-month delay whilst they resit an English language test.
However, it’s your responsibility to ensure that you are eligible for registration. So you should also be checking these things yourself.
It’s hard to fathom given the amount of communication from health departments, medical schools and student colleagues. But every year there are a handful of medical students who forget to apply for their internship. This means having to wait another year. Don’t let that be you.
Dr Anthony Llewellyn | Career Doctor
Tip #3. Research and Apply Early.
It’s hard to fathom given the amount of communication from health departments, medical schools, and student colleagues. But every year there are a handful of medical students who forget to apply for their internship. This means having to wait another year. Don’t let that be you.
There are even more students who leave their applications to the last minute. Only to find that they are missing a vital document. For example, this could be evidence you need to substantiate that English is your first language, such as a high school certificate. Or perhaps your last name has changed whilst you have been in medical school? Or maybe you need to submit a CV with your application?
As soon as the application page opens for each State and Territory you are going to apply to make sure your register. And then go as far through the process of applying as possible so you can see if there is some sort of document you need to obtain.
Tip #4. Practice Your Video Interview Technique.
If you are one of the many students who may need to undertake an interview for your internship choices as occurs in certain situations, such as rural preferential recruitment and certain States such as Victoria. Then you should be prepared for the fact that this year your interview is unlikely to be held in person and very likely to be conducted on video.
There’s a lot more than you think to video interviewing. For a rundown on this check out this recent post.
Tip #5. Know Where You Sit In The Priority List.
ts important to know where you sit on the priority list. Each State and Territory has a slightly different order but in essence, it goes something like this:
If you are an Australian Citizen or Permanent Resident and went to Medical School in that State or Territory you are top of the list.
If you are an Australian Citizen or Permanent Resident and went to Medical School in another State or Territory or New Zealand you are probably second.
If you are an International student who studied Medicine in Australia you are probably next.
Tip #6. Know the Key Dates, including Offer Dates.
As noted above it’s crucial that you know the key dates. If you miss your application submission date (and it does happen) there is no allowance for a last-minute submission. You also need to make sure you are available to accept your offer. Generally, the window for offer acceptances is quite narrow (often 48 hours).
For this year the day on which the first round of offers can be made nationally is 12th July and most offers will come out on that day. Thereafter there is a series of offer windows for 2nd and 3rd and 4th rounds etc… in between which there is a mandated pause, which allows the National Intern Audit process to run. This is a system that works to ensure that vacancies are being freed up as soon as possible by highlighting medical students who may have an offer in more than one jurisdiction and ensuring that they accept one offer and decline others.
Priorities Within Priorities.
Some States and Territories also have priority pathways to ensure that groups such as Aboriginal and Torres Strait Islanders and doctors who wish to work rurally or regionally can obtain their preferred placement early.
So if you are an International student and like the idea of working rurally it’s probably a good idea to consider a rural pathway as it will likely boost your chances of gaining an Intern position earlier in the process.
The Commonwealth – Junior Doctor Training Program Private Hospital Stream
Intern Positions TBD
The information below is for the previous year.
Annual Salary = will depend on which State or Territory you are employed in.
The Commonwealth provides an additional Internship program for international students who study at Australian medical schools.
*Any excess posts may be applied for by other IMGs in Australia
The main function for this program over the years has been to provide additional opportunities for international students studying Medicine in Australia a chance to complete their internship. This is done by tendering to various private hospitals for additional intern positions.
The program was retitled in 2020 to the Junior Doctor Training Program Private Hospital Stream when there were 115 positions on offer.
Normally there is not as much information about the program available until a mad flurry at the end of the year. And 2020 seems to be no different. They are still sorting out which hospitals will provide internships. After which there will probably be some information about how to apply.
For now we know that the eligibility requirements are that you must either be an international full fee-paying medical graduate from an onshore Australian medical school. This is Priority One. If not all positions are filled by priority one medical graduates then the private hospitals may then recruit other medical graduates who have provisional registration. This is the Priority Two category. I am not sure how this priority category two helps any IMG as they must already have provisional registration. I guess it might help some IMGs already employed and on the standard pathway jump into a better training program.
Eligibility Requirements for Intern (PGY 1) Junior Doctor Training Places under the Junior Doctor Training Program Private Hospital Stream
Under the PHS, participating private hospitals must prioritise international full fee-paying medical graduates from onshore Australian medical schools (Priority One). Should these places not be filled, private hospitals may then recruit other medical graduates eligible for provisional registration (Priority Two). This means that the Commonwealth Scheme provides one of the few opportunities for IMGs who are applying via the standard pathway process to gain an internship position in Australia.
To do so you will need to have met the Medical Board of Australia provisional registration requirements as a medical practitioner. And also have met the English language proficiency requirements for registration purposes. And commit to obtaining an appropriate visa to work in Australia during the internship year. Private Hospitals funded to deliver the Private Hospital Stream from 2020-2022 are: – Mater Health Services North Queensland (delivering PGY1 places) – Mercy Health and Aged Care Central QLD – Friendly Society Hospital, Bundaberg; Mater Private Hospital, Bundaberg; Bundaberg Base Hospital, Bundaberg; – — — Mackay Base Hospital, Mackay; Mater Misericordiae Hospital, Mackay (delivering PGY1, PGY2 and PGY3 places) – MQ Health (Macquarie University Hospital) (delivering PGY1 places) – St John of God Ballarat Hospital – Grampians Intern Training Program (delivering PGY1 places) – Mater Hospital Sydney (delivering PGY1 places) – St Vincent’s Private Hospital Sydney (delivering PGY1 places) – Ramsay Health Care WA (Joondalup) (delivering PGY1, PGY2 and PGY3 places) – Greenslopes Private Hospital (delivering PGY1, PGY2 and PGY3 places) – Calvary Health Care Riverina (delivering PGY2 places)
There are lots of considerations when it comes to putting in your Intern application. Everyone is a bit different. Some graduates feel like they would like to be close to home and family whilst going through their transition to Intern. Others see it as a chance to get away and explore a new place and location. And then others focus on the long-term career prospects of certain locations.
I think this last consideration is a little overrated for most. You can generally experience a wide range of medicine in your first couple of years of medicine after graduation and there is scant evidence that this affects your prospects of applying for specialty training posts.
That being said if you have an interest in anything other than Medicine, Surgery or Emergency Medicine as a future career you should probably investigate whether this particular specialty is offered at the hospitals or networks to which you apply.
Unfortunately, the internship model in Australia is quite antiquated and we have continued to use the experience as a proxy for competency when a large portion of the medical education world has moved on. The result has been the mandating of the 3 core terms for internship of Medicine, Surgery, and Emergency Medicine. There is really no solid educational basis for this approach and one of the unfortunate outcomes is that all the other specialties get squeezed out and few interns get to experience psychiatry, general practice, obstetrics, paediatrics, pathology etc… which ultimately does have an effect on recruitment to these specialties.
So the basic message is this. If you are really dead set keen on doing radiology as a career you should try to track down the very few locations that might offer this rotation to either interns or residents.
Each year the Australian Medical Students’ Association produces a very useful Intern Guide with lots of information about the composition of intern training networks across the country. The 2020 version did not appear to eventuate. So I can only assume they are no longer compiling this. But here’s a link to the 2019 version.
Related Questions
What If I Have Special Circumstances Which Make It Hard For Me To Work In Certain Places?
All States and Territories Have processes for considering special circumstances. Some of the types of circumstances that are generally approved are: where you may have certain health conditions that mean you need to be close to certain hospitals or specialists; where you have dependents, such as young children, and are unable to relocate due to care arrangements; and where you and your partner want to work as doctors in the same location. Generally, requests to stay in certain locations, for reasons such as work commitments of partners or needs of school-aged children are not granted.
I Have Received My Intern Offer. But I Would Like to Defer It. Is This Possible?
This will partly depend on how long you wish to defer for. If you just wish to defer for a a few months. Once you have your offer and are in discussions with your new employer make enquiries. It may be possible to negotiate a later start with your employer. Most employers will generally prefer that you start on time, so that you are not out of sync with your colleagues. But there might be some advantage for the employer in you attending orientation but then starting a bit later as it will probably help them to fill out roster gaps. On the other hand. If you wish to defer for a complete year. Then you will need to check the policy of the State or Territory that has provided you an Intern offer. In some cases (for example Victoria) you will be permitted to defer and your place will be held for you the following year. In most other cases you will need to reapply the following year and check whether your priority status has altered. In most cases you have the same priority status. Also bear in mind that it is unclear how long you can defer commencing your internship. However, the eMedical Board of Australia expects that once you have commenced your internship you will have completed this process within 3 years.
I Am a Doctor With a Medical Degree From Outside Of Australia. Can I Apply For Internship?
Unless you obtained your medical degree from a New Zealand Medical School. Then the brief answer to this question is no. I would love to stop there. And I really think you should as well. But there are rare circumstances where you may be able to obtain an internship with a medical degree from outside of Australia. But the Medical Board of Australia strongly advises against this option and so do I. For good reasons. Firstly the whole Australian medical internship system is designed to ensure that Australian medical graduates are able to undertake an internship. Not for overseas graduates. Secondly (and as a result of the first point) it is very rare to be offered the chance. Some States and Territories will not even consider an application from an IMG for internship. Others will only do so in limited circumstances, for example, the Northern Territory will accept applications from IMGs who may have done a medical student elective or clinical observership in the Northern Territory and who have experience in rural, remote and indigenous health locations. But even then these applicants are at the bottom of the priority list for obtaining an internship. South Australia will accept applications. But again you are bottom of the list. Queensland will also accept applicants, but only if you have never worked as a doctor. And again you are bottom of the list. A final note on this question is that the majority of IMGs who do obtain a medical internship position each year in Australia generally have Australian citizenship or permanent residency.
I Have Heard That Some Graduates Miss Out On Internship. Is This True?
Whilst it is theoretically a possibility that some medical graduates miss out on Internship according to information provided by HETI for the most recent year of intern applications no-one was actually left at the end of the process without an offer. Only Australian citizens and permanent residents are guaranteed an intern position under the COAG agreement. However, there are generally enough intern positions available for those students who have come to Australia to study medicine and the Commonwealth Private Hospital program offers additional spaces for those that may miss out. That being said. It is also clear that many graduates choose to drop out of the application process themselves. So not everyone who applies gets an offer. The assumption is that some graduates take up similar intern opportunities in other countries upon graduation.
I Am Not an Australian Medical Student. How Do I Obtain an Intern Placement Number?
In this situation you do not require an IPN and will not be issued with one. You can still apply for internships. But unless you are a New Zealand medical student your chances of gaining a place are very very limited.
(Disclaimer: all information here has been sourced in good faith but things do change so you should always do your own due diligence in such matters, we are providing this information to aid you in your application but take no responsibility for any outcomes)We’d welcome feedback from any Intern programs in relation to the accuracy of the above information.
This post is specifically about addressing employment gaps on your resume. There are several posts online talking about how to explain employment gaps in your resume in an interview. But surprisingly nothing of great quality about how to actually write these up on your actual CV or resume.
It is critical that you do acknowledge employment gaps in your resume. Here’s what you need to know:
If you are a professional such as a doctor, employers expect a full work history so any employment gap is going to be obvious to a trained eye.
It is best to list gaps in the appropriate spot in the chronological order of your work history.
If your gap was for personal or family reasons, such as having children or caring for a loved one. All you need to do is write the date of the time off work and “personal reasons” or “family reasons”
Some gaps, for example time off to study or time off to do volunteer work might merit a little bit more information, particularly if they enhance your employability
If during your “gap” you have actually been working in another type of job. Then you don’t actually have a gap. You should just include this work in your work history. Despite what you think it will be seen as a good things by employers in countries like Australia.
So you are probably wondering at this point, why do you need to address an employment gap in your CV or resume? Let’s dig into that a bit further. And then go over the most common scenarios where you might see employment gaps on resumes.
Why Gaps On Your Resume Are Important to Address.
In a job such as medicine, it is a big deal that you tell the truth and a requirement that you do not lie on your resume. Whilst it’s possibly a bit of a grey area, omitting things of substance, will not generally go over well.
When someone from a selection panel reviews your resume and sees a big hole in it between, for example, your resident year and your senior resident year. They will wonder why this is the case. They will wonder whether something bad happened, such as you being dismissed from your post for performance reasons.
You don’t want to leave this hanging in the air.
The problem, of course, is that many of the reasons for taking time off in a job such as medicine are not related to your work or employability, but other things that you are passionate about in your life. And some of these things can bring into scope the issue of job discrimination.
So how do you best deal appropriately with this situation?
Where Do You List Gaps In Employment On Your Resume?
I generally recommend that you do this in the most obvious place, the employment history section. In the appropriate place, i.e. between the job before your time and the next time you were employed. This makes it easy for the person reviewing your resume to find and comprehend.
If, however, you feel that this might detract from the look and feel of your work section you can alternatively add another heading in your resume entitled “Gaps in Employment” and then list your gaps here.
I tend to advise my clients against this as it’s drawing more attention than is necessary.
So. Now we know where to write up gaps on your resume. Let’s talk about how to write about the specific types of gaps.
What to Do If Your Resume Gap Is Due to Having Children.
Questions and information about your family are an off-limit area for your prospective employer. Whilst being a good Mum or Dad is definitely a translatable skill. For these gaps on your resume, you are best off not providing any further details.
Simply write something like: “family reasons” or “family leave” or even something less specific such as “personal reasons”.
What to Do If Your Resume Gap Is Due to Caring for A Family Member.
Similar to having children. Your prospective employer does not need to know the details of your child caring arrangements or sick relative. Once again for these gaps on your resume, you can just simply indicate that the time off was for “family reasons” or “personal reasons”.
What to Do If the Gaps On Your Resume Are Due to Travelling.
The desire to take time off to travel is understandable to most employers. In most situations, your vacation probably didn’t result in you obtaining a new skill related to your employability. Even if you personally feel your trip to South America effectively dealt with your burn-out. So for these gaps on your resume, you can just say something like “time off to travel”
What to Do If the Gap On Your Resume Is Due to Study.
In most cases, the study you are undertaking will have some form of relevance to your medical career. So here it’s worth spending a few words explaining your time off to study.
For example, you may have taken 6 months off to prepare for your major examinations. So you might write something like: “I took 6 months of approved leave from my post in order to prepare effectively for the [insert name of college] written examinations.”
As another example, your time off might have been to help complete a formal degree course that will advance your career. So you might write something like: “I took 6 months of approved leave in order to finalize my Masters in Medicine, including the publication of 2 research papers.” Remember, you will want to also spend some time explaining your formal study in the Education section of your resume as well.
What to Do If the Gap On Your Resume Is Due to Volunteering.
In general, volunteering work will be seen as commendable by prospective employers. And the experience is likely to have left you with some additional skills in terms of the general capabilities required of a doctor. For example, if we take the CanMEDS framework, volunteer work is likely to tick a number of boxes, including communicator, collaborator, and health advocate.
So again for these particular gaps on your resume, it’s generally worth spending a few lines to provide some information about your volunteer activity.
For example: “During this period of approved leave I took time to work with an NGO in East Timor, where I was involved in the establishment of a new primary care clinic, the experience taught me some vital lessons about communicating across cultures different to my own and working with different types of health and non-healthcare team members, including roles that I would not normally come across in Australia, for e.g. health promotion officers.
What to Do If the Gaps On Your Resume Are Due to Moving Countries.
The process of moving country and re-establishing oneself in the local medical profession takes time. This is understood by employers. Generally, during this time you are not just moving country but also studying or preparing yourself for the examinations required to become a doctor in that country.
So for these sorts of gaps on your resume, if we take an Australian example you might write something like:
“During this period of time, I migrated to Australia and prepared myself for the Australian Medical Council exams. I also undertook an observership at Hospital X.”
Are the Gaps On Your Resume Really Gaps?
One final thing to consider is whether that gap on your resume is indeed a gap?
This is particularly the case with IMG doctors. Because often the gap is not because they are not working but just because they are not working in medicine. IMG doctors in Australia often take up other forms of employment whilst getting reaccredited in the country.
So you should really just write this up as another work experience on your resume. It is not seen as a bad thing by Australian employers. On the contrary, it’s a sign that you are at least employable in Australia and can work in a team.
And there are generally more skills that you can demonstrate out of such experience.
Related Questions.
My gap in employment was a few weeks between jobs. Do I need to address this?
No. If your time between jobs was only a few weeks, then it’s not necessary to specifically indicate this on your resume.
2020 was an unusual year. That’s obviously an understatement. Despite all the pandemic concerns the need for doctors to be helped with their doctor job applications remained ever-present. Possibly prompted a little bit by the advent of video interviewing. In 2020 I clocked up 437 coaching hours, including my first group interview coaching session. This was a highlight for me as all 3 candidates gained entry into the highly competitive RANZCOG program. So. We’ve prepared this reference for you for medical recruitment 2021 to help you make the right choices.
If you are preparing for a new job in medicine in 2021 then here is a summary of what we at AdvanceMed advise that you should be doing right now:
Keep an eye on the main annual medical recruitment portals. We don’t anticipate as much disruption this year. But its always good to know your timeline as well in advance of time as possible.
There are plenty of things you can be doing now to prepare yourself for your next career move in medicine, regardless of whether there is a clear application date, these include preparing your resume, gathering referees and beginning the process of interview preparation.
The majority of interviews this year are likely to be again conducted via videoconference, therefore, its important to invest some time and effort preparing to interview on this medium.
Let’s now look at some of these issues in more detail including the key things you can be doing now to be present the best version of yourself on the day.
How Best To Prepare Yourself for Medical Recruitment 2021.
What key advice do I have for medical trainees who would like to know how they can prepare themselves for medical recruitment in 2021? Here are my top 5 tips.
1. Enact Your Medical Selection Plan Now.
There’s no reason to wait if you know that you are going to be going for a new job this year. Annual medical recruitment is likely to be one of the most important events of the year for you. You should be enacting the first part of your plan now if you have not already done so. Make sure you find out as soon as the jobs portals and timelines open when you will be able to apply and when your interview is likely to be.
Even if you are a bit uncertain. Perhaps you are an IMG doctor who thinks they might get an interview opportunity. But doesn’t really know. You should not wait till the interview call to start preparing. Because by then it’s likely to be all too late for you. Start putting the preparation in now.
Of critical importance to your preparation will be your Resume. There’s plenty of advice on this blog about how you can make this document stand out. You should be aligning this with the competencies being sought for the position/s you are intending to apply for. Think about adding in a story about COVID-19 that shows off one of these competencies. Ensuring that you have relevant, recent, and diverse referees to speak on your behalf is also something you can be doing now.
You should also be thinking about starting your interview preparation and medical interview coaching if you are intending to use a coach. Many candidates that I coach start this process far too late. In my experience, there is little risk of starting too early (you can always pause for a bit if you lose momentum). Interview skills are like muscles. They need regular training to help you show your best on the day. The problem is. If you haven’t interviewed for a while. This muscle is likely to have atrophied.
2. Practice
This is the most vital tip in my opinion. You should definitely treat the interview as an examination or a performance. I’m betting that throughout medical school you practiced and prepared for exams. So why would you expect to just turn up for your next job interview, “wing it” and turn in a great performance?
Your next job in medicine is just as important, if not more important than getting a pass on an exam. So you need a bit of a practice schedule and you need to actually practice. I recommend giving yourself at least 6 weeks if possible and do at least one practice session per week prior to your actual interview. If you have less notice of your interview then obviously you will need to condense this and increase the frequency. Better yet. If you are anticipating a new job in the next 6 months. Think about setting up a practice schedule now.
3. Find out what the panel is looking for
You need to understand what the interview panel is looking for. So you can practice the right questions and prepare the right examples. I’m often asked by doctors.
“How can I predict what sorts of questions I will be asked?”
Well. It’s actually a lot easier than you think.
The questions you get asked in the interview should relate to the Selection Criteria. So to find these go to the appropriate section on the job description and review it. They are usually placed towards the end of the document. These should give you a fair indication of the types of questions you will be asked.
Sometimes, particularly for college selection, rather than selection criteria, there is a competency framework. These are normally easy to find on the college website. Again these will give you a very good guide to what you will be asked about.
You can then generate appropriate questions or there are places online you can find a bunch of them. You can access our free question bank here.
4. Review your CV for examples.
Your CV or resume is a treasure trove of achievements from which to draw upon examples of your past work (or at least it should be). Review your CV for examples so that you can use these as part of your answers to questions when you engage in the annual medical recruitment process.
Remember providing an example from your past work is extremely powerful at the interview.
Dr Anthony Llewellyn, Career Doctor
Sometimes you will be asked for an example as part of a behavioural question. But don’t be afraid to offer one, even if the question is a hypothetical question.
You are basically telling the panel.
“I can do this. Because I’ve done it before.”
And panels know that past behaviour predicts future behaviour so they will value this information.
5. Review Your Video Conference Set-Up
It’s important to understand that your next doctor job interview is most likely to be conducted on something like Zoom. There are significant differences in interviewing on video versus in person. Both from a technical perspective as well as from a practice perspective.
You should definitely be reviewing and modifying your videoconference setup and your environment as well as actually practising interview questions using video. The latter is actually a good idea in general as it affords you the chance to record and review your performance.
Why do I say that you need to record yourself and watch yourself back? Well. Interviews are as much about body language and tone of speech. In fact even more about these things. Than what you say.
So. It’s important to know how you appear during an interview.
The only way you will know this is to observe yourself.
Here’s a great example:
Often when I am coaching candidates for an interview I notice that they appear quite stiff in their presentation. This is normally because they are trying to control their hands. By sitting on them or anchoring them in their lap. Actually, you generally want to let your hands get involved in your interview performance. Once we fix this problem. The visual performance always looks a lot better.
There are a number of options for filming yourself for an interview performance. My recommendation would be to use a desktop or laptop set up and record yourself on Skype or Zoom. This way you should easily be able to get at least a head and shoulders view of how you look whilst seated. It’s particularly important to be able to see what you do with your hands.
Alternatively, you can use your smartphone with a tripod if you have one or even just a stack of books on the table. Selfie videos are not as good as you have at least one hand engaged for the filming purpose. Similarly observing yourself in the mirror is not as good as you cannot rewind and go back.
7. Engage an Expert
My final tip is to get some interview practice with an expert.
What do I mean by an expert?
I mean anyone who has had significant experience being a member of a selection panel and/or experiences in coaching candidates for interviews.
Preferably both.
So as a minimum. Try and get someone like a Director of Training or Director of Medical Services to give you a couple of sessions. These people have generally sat in on hundreds of interviews.
Don’t fall into the trap of relying on feedback from fellow candidates, your family, or friends. Their feedback is likely to be unhelpful and too much on the positive and encouraging side. Because they have no context for what the panel is looking for and they are too invested in your success and you as a person. You want as critical feedback as possible.
And. If you want to up your game and performance to a higher level.
The most obvious reason is that interview coaching can help increase your chances of getting a job. There are a number of ways this can occur.
Coaching can help you overcome any nerves or anxiety you have about the process. Coaching gives you a chance to experience answering many different interview questions. Coaches provide you with feedback to help improve your responses during interviews. The more you practice with a coach, the more confident you will become. By engaging with a coach you are also ensuring that you commit to your own practice regimen, which is important for a good performance.
Some reasons you may want to consider engaging a doctor interview coach.
It’s been awhile. If it’s been a few years since the last time you interviewed for a doctor job or if your last interview was fairly simple and you anticipate this one will not be the same, then a coach can help you rehearse and regain your interview confidence.
You get nervous before interviews. A little bit of anxiety is good going into an interview. But too much anxiety can affect performance. Practicing with a coach can help you feel more comfortable, relaxed and prepared.
You get interviews, but not offers. Often its difficult to get honest feedback from medical interviews. A coach may be able to help work out what is going wrong for you.
You are not sure about something on your CV. Maybe you have had to have a break in work. Or your last job didn’t go so well. Are you perhaps switching specialties. A coach can help you with how to tell the right story in relation to these sorts of issues.
Its your dream job and you want to land it. A coach can help with feeling confident in these situations.
On the other hand, if you’re a confident interviewer and have always tended to perform well during interviews, then a coach may not be necessary.
Types of Interview Coaching
There are many types of interview coaching. Some coaches meet with you in person, and others speak with you online or on the phone. In general interview coaches work on something called “performance coaching”. Think of it like a sports coach working with an elite athlete. A key element is practice with feedback. The more practice and the more immediate the feedback the better.
If you meet the coach in person or online, they can also help you develop effective visual communication. The coach can work with you on facial and body expressions that convey trust and show active listening.
Coaches may also help you with other elements of the interview, including how to ask the right questions of the employer, how to research the job and the panel, and even some advice on how to dress.
How to Find a Doctor Interview Coach
There are lots of coaches available to choose from. Career coaches often offer interview coaching. Some things you should consider in a coach are the following:
What is their training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process. Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Do they provide face to face coaching or on the phone or online. Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session. Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
Whilst doctors from the United Kingdom and India are generally more frequently encountered in Australia. It is not unusual at all to come across a doctor from Ireland who is now happily working in Australia. Whether this is for a short-term working holiday or a permanent move. As someone who has worked in Medical HR for more than two decades, I have found that Irish doctors on the whole to be a really good group to work with.
Can doctors from Ireland find employment in Australia? The answer is, of course, yes. The Republic of Ireland provides a significant but steady source of overseas doctors or International Medical Graduates (IMGs) working in Australia. Of course, no doctor coming from another country is absolutely guaranteed to be able to work in Australia. But if you are from Ireland you have a very good chance.
Because the Irish medical training system is recognized by the Medical Board of Australia as being on par or what is termed “competent”, Irish doctors have good success with either becoming generally registered through the competent authority pathway or being recognized as a specialist through the specialist pathway. In 2019 (the latest year we have figures for) 263 doctors from Ireland applied for provisional registration in Australia with 257 of those applications granted. That is on top of the hundreds of Irish doctors already working in Australia.
So the prospects for working in Australia as a doctor from Ireland are positive. But it’s important to have a bit more detail. As I have highlighted there are two main options for getting registered. So we will talk about these first and then go into some other common questions.
The Competent Authority Pathway. The Trainee Option For Ireland Doctors Australia.
If you are a trainee doctor in the Republic of Ireland. Then you are looking at the competent authority pathway for working in Australia.
The competent authority pathway assigns a preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States and the Republic of Ireland.
There is largely a historical rationale for this situation. It is based on the premise that all these jurisdictions have similar approaches to medical school training and similar standards.
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools, the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically as those from Australia.
If you are an international medical graduate (IMGs) and you have achieved general registration in the United States, Canada or the United Kingdom (but not the Republic of Ireland) you are also eligible for the competent authority pathway.
So it is important to note here that there is no competent authority pathway for IMGs to gain full registration in Ireland and then attempt to gain registration in Australia. You have to have graduated from a medical school in Ireland.
What are the steps involved in the competent authority pathway for Ireland Doctors Australia?
The key steps are as follows:
Securing an employment offer
Applying to the Australian Medical Council for primary source verification
Applying for registration to the Medical Board of Australia
Completing 12 months supervised practice
Applying again to the Medical Board of Australia for general registration.
Eligibility for Competent Authority
You can do a “self-assessment of your eligibility for the competent authority pathway on the Medical Board of Australia website here.
The essential requirements are:
You need to be a graduate of a medical course conducted by a medical school in the Republic of Ireland which is accredited by the Medical Council of Ireland (MCI).
(Of note this now includes off-shore courses which are accredited by the MCI which, as of the writing of this post included 3 courses run by the National University of Ireland in Malaysia (x2) and Bahrain.
AND
Successful completion of an internship in Ireland (Certificate of experience).
What types of jobs can I apply for as an Irish Trainee Doctor in Australia?
You can pretty much apply for any sort of trainee job. There are often a number of postgraduate year 2 or 3 general jobs on offer. They are generally termed Resident Medical Officer in most States and Territories, but may also be called House Officer or Hospital Medical Officer in some places.
Above these sorts of posts, come the specialty training positions. Australia’s specialty training system is fairly much in parallel with the Republic of Ireland. So you tend to enter specialty training around postgraduate year 3. These positions are generally referred to as Registrar positions. But you might also see advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most jobs you come across will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice, the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
your previous experience, especially in the type of position for which you have applied
whether you have practiced recently and the scope of your recent practice
the requirements of the position including the type of skills required for the position
the position itself, including the level of risk, the location of the hospital or practice and the availability of supports (supervisors)
the seniority of the position, for hospital position
In general you will either be approved for Level 1 or Level 2 Supervision. There are 4 Levels and the higher up you go the less direct oversight you require.
Level 1 Supervision.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times and you must consult with them about all patients.
Remote supervision (for e.g. by telephone) is not permitted. This type of supervision is generally recommended when you are very junior yourself or entering a junior role which you are not very familiar with. In Australian major public hospitals, there are many layers of other doctors who you can get supervision from. So Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision.
Level 2 Supervision, which is what most Irish trainees will normally be approved for is a step up from Level 1 Supervision.
Supervision must primarily be in person but your supervisor can leave you to do work on your own and you can discuss by phone. You should discuss with them on a regular (daily) basis what you have been doing with patients. But do not need to discuss every case.
Level 3 Supervision.
Level 3 Supervision, is what you might receive if you are working in an Advanced Trainee role in Ireland and transferring to something similar in Australia. In this case, you have much more primary responsibility for the patient. Your supervisor needs to make regular contact with you but can be working elsewhere and available by phone or video.
What happens after I commence my position?
Once you are approved for registration and you have your visa issues sorted you will be able to commence work. Generally, your employer helps you out with all these things. You will be working under what is called “provisional registration” by the Medical Board of Australia.
Generally, all you need to do for these 12 months is to pay attention, show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia and it is your responsibility, not theirs to see that they are completed and returned on time. If all the reports go well you will be able to be recommended at the end of the 12 months for general registration.
You will probably be starting to look for another job or negotiating an extension around this time. With general registration, you may be able to apply for a skilled visa, as well as be looking at applying for permanent residency.
Permanent residency is crucial for applying for most specialty training programs. See below.
The Specialist Pathway. The Option For Irish Specialists
For qualified specialists from Ireland, your option for working in Australia is what is called the Specialist Pathway.
Actually, it’s a combination of the Specialist Pathway and the Competent Authority Pathway. More on that in a bit.
Once again your process starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need Position, in which case the employer or recruitment agent will provide you a lot of support and will likely pick up the costs of being assessed.
For most International Doctor specialists however these days you will be approaching the college directly to be assessed for specialist recognition. This is not something to be trifled with. The paperwork requirements and the cost (generally around $10,000 AUD or more) is considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
Finding Out What You Need To Do.
We have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The majority of Irish specialties (but not all) map to a similar college or specialty in Australia. So working out which specialty goes into which Australian college is generally not too confusing. We have put together a summary of the Australian specialist medical colleges here.
After you go through your specialist assessment you are given an outcome.
In the majority of cases for Irish specialists, you will be deemed substantially comparable. This essentially means that you will need to work under some form of peer review for up to 12 months and so long as your reports are satisfactory you will be recommended for specialist registration at the end.
Occasionally specialists from Ireland are deemed to be partially comparable (a situation where this may occur is if you have just recently finished specialty training but have not worked as a specialist for very long). In this situation, you will need to work under supervision for longer and may well also face some formal examinations.
Rarely are specialists from Ireland deemed not to be comparable by the college. This only happened to 1 out of 31 specialist doctors from Ireland in 2018. If you are deemed to be not comparable, this means you cannot directly become a specialist in Australia. You will probably have to go through the competent authority route and re-enter training in Australia.
How to Maximize Your Chances of Getting a Substantially Comparable Outcome.
To ensure that you are seen as substantially comparable by the relevant college I would recommend the following:
You should have your Certificate of Satisfactory Completion of Training and relevant college Fellowship and be registered as a specialist with the Medical Council of Ireland
You should ideally have worked substantively at a Consultant level in your field for 2 years or more
You should be able to demonstrate good standing with the Medical Council of Ireland and your employers
You should be able to demonstrate ongoing continuing professional development
You should prepare for your interview with the college as if it were an important job interview
Specialist Pathway Course
Free Course
You can enrol now in this free course that will step you through all the requirements for working as a specialist doctor in Australia
Can you enter training in Australia if you are a doctor from Ireland?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in many cases permanent residency or citizenship.
After receiving your general registration doctors from Ireland can apply for specialty training in the same way that Australian trained doctors do. And if accepted will go through the exact training program and experience. Some colleges may offer recognition of prior learning for training you have done already. But this varies and may at best normally shave one or two years off of your training.
An Alternative But Limited Option.
There is an alternative but time-limited pathway for Irish doctors who are just seeking a short term experience in Australia to add to their training in Ireland. This is called the Short Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in Ireland or be less than two years from completion. So this is a program mainly for early-career specialists or advanced trainees.
In this pathway, you go through the same steps with the AMC as per the competent authority pathway to gain registration. You will not, however, be able to apply for specialist assessment as part of this pathway. But if you gain general registration you may then be able to apply for another position and then apply for specialist assessment.
How many doctors from Ireland are working in Australia?
There is no one public data source to tell us how many Irish doctors are currently working in Australia.
From data collected by the Australian Government, we know that for 2018 and 2019 (latest available years):
In 2018, 263 applications were made for provisional registration via the competent authority pathway by doctors from Ireland with 257 granted provisional registration.
In 2019, 39 applications were made for specialist assessment, 8 were withdrawn prior to full assessment. Of the remainder, only 1 was deemed not comparable, 10 partially comparable and 20 substantially comparable.
In 2019, 13 out of 13 specialty doctors from Ireland were recommended for specialist recognition.
Costs of Moving To Australia and Working As a Doctor.
There are lots of costs to consider when thinking about moving to Australia to work as a doctor.
There are some direct costs to consider. Most of which relate to the bureaucratic process of being assessed and gaining registration.
Some of the costs you may be up for, include:
AUD (unless other wise noted)
Establish Portfolio with Australian Medical Council
$500
Registering with EPIC and having one primary degree checked
$125 USD + $80 USD
Medical Board Application Fee for Provisional Registration
$382
Medical Board Application Fee for Specialist orGeneral Registration
$764
Medical Board Provisional Registration Fee
$382
Medical Board General or Specialist Registration Fee
$764
College Specialist Assessment Fees
$6,000-$11,000
College Placement Fees (for the period of supervision)
$8,000-$24,000
Further, if you are required to undertake further exams there will be a cost for this as well. As an example, RACS charges an exam fee of $8,495.
The Cost of Your Time and Effort.
To all of this cost, you will need to factor in the cost of your own time. It takes a lot of effort and persistence to deal with the paperwork and track down the records you need.
In addition, you are probably going to have to pay costs in your own country for things like records of schooling and certificates of good standing.
There are also visa costs.
And then there is the cost of airfares and transporting your belongings halfway across the world.
Depending on where you work in Australia you may find that the cost of living is higher or lower than you are used to. House prices and therefore house rental rates have gone through the roof in Australia in the last decade or so but are starting to come down.
You will probably have to factor in some initial extra hotel or short term rental charges whilst settling in and you may find if you have children that you have to pay to enrol them in school as public schooling is only generally free if you are a citizen or permanent resident.
If you are lucky and in one of the specialty areas of demand your employer may offer to pay for some of these costs. It’s certainly worth asking about it.
We hope that you found this summary about how Irish doctors can work in Australia useful. If you have any questions or queries or just want to relate your experience. Please feel free to leave a comment below. We would love to hear from doctors from Ireland who have made the journey to Australia.
Related Questions.
Do I Need to Sit An English Test?
Doctors from Ireland are amongst a select group of countries for which the Medical Board does not expect an English proficiency test. However, there may still be some circumstances where you do need this. If, for example, some of your schooling was in another country. You should always check the requirements.
Are there any other options for working as an Irish doctor in Australia?
Some doctors just want to come to Australia for a limited period of time as an opportunity to train in another country.<br>As we have highlighted above there is an alternative but time-limited pathway for US doctors who are just seeking a short term experience in Australia to add to their training in the US. This is called the Short Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in the US or be less than two years from completion. So this is a program mainly for early-career specialists or advanced trainees.
Should I use a medical recruitment company if I am considering working in Australia?
It is possible to deal directly with employers in Australia as an Irish doctor. In general, however, when moving from one country to another most doctors find it useful to engage with a medical recruitment company as they can tend to take some of the stress out of the planning for you and help with all the paperwork and negotiating with prospective employers. Some medical recruitment companies also provide migration services and relocation services as well. We have written more on this subject
Can you do your internship in Australia as a doctor from Ireland?
Basically no. Internship in Australia is a provisional year that only applies to medical graduates from medical schools in Australia and New Zealand. There is a \”loophole\” which only applies to doctors who have not been able to complete an internship or equivalent in their own country. But the Medical Board warns that this is not a great option and is only granted in limited cases. You are far better off applying for Intern training in Ireland and completing this year first.
How hard is it to become a specialist in Australia if you are from the Republic of Ireland?
Specialist doctors from the Republic of Ireland are not automatically granted specialist recognition. However, most are. As you can see from above in 2019 there were 39 applications made for specialist assessment to the Australian colleges by Irish doctors and of these, the majority were deemed substantially comparable. Irish doctors tend to get a very favourable outcome in comparison to doctors from most other countries. Ireland has generally one of the highest rates for doctors being seen as substantially comparable.
Are there any particular specialties that are easier to apply for?
The majority of specialties have some vacancies and will provide opportunities for Irish and other IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be quite difficult. On the other end of the spectrum general practice, psychiatry and most parts of critical care medicine are often always looking for doctors.
Recency of practice is an important concern for medical practitioners in Australia. It’s something you must address both when you register with the Medical Board of Australia for the first time, as well as each time you apply for re-registration. Most doctors tend to focus on the Medical Board standard in relation to recency of practice. But you will also find that most employers have their own expectations and standards around recency of practice. In this post, I am going to guide you through what you need to know about recency of practice, so that you can be appropriately addressing this issue both with the Medical Board as well as with employers.
So, firstly let us define what we mean by recency of practice for doctors in Australia. According to the Medical Board of Australia, every registered medical practitioner is required to demonstrate recency of practice, which is defined as working a minimum amount of four weeks full time within your scope of practice in one year (one registration period) or 12 weeks full time within your scope of practice across 3 years (3 registration periods).
From an employment perspective, whilst employers need to be mindful of the Medical Board standard they will generally apply their own standards. A good rule of thumb is if it has been more than 2 or 3 years since you have done a significant amount of clinical work this may be seen as a negative by a prospective employer.
So, in the rest of this post, we will discuss some of the finer details of the recency practice standard, what might happen if you are found to not be recent enough in practice as well as the options for addressing recency of practice from both a Medical Board as well as employer perspective.
Why have a recency of practice standard?
It is important that doctors remain current in the type of clinical medicine that they practice. Most laypeople would consider a situation where a doctor had for example not practiced medicine at all for 5 years and not engaged in any continuing professional development during this time as one where such a doctor may pose a risk to the public if they were to return to clinical medicine with no initial support or oversight.
The question, therefore, is how much recency of practice is enough? Interestingly the Australian Health Practitioner’s Regulation Agency (AHPRA) which oversights the National Boards, including the Medical Board, has reviewed this question a few times. In their most recent report they comment that:
Research undertaken for this and previous reviews of the ROP registration standards did not provide a definitive answer to the question of how much recent practice a health practitioner needs to maintain their skills and knowledge, or whether minimum hours to maintain competence vary according to the profession, type and scope of practice. National Boards have drawn on the research that is available as well as their regulatory experience and the experience of other National Boards to set requirements for recent practice.
AHPRA 2019 Report
They concluded that the revised registration standards balance public safety versus the regulatory burden of allowing practitioners some level of flexibility in their working arrangements.
Scope is just as important as recency.
It is important to note that the Medical Board still expects doctors to recognise their own limitations. Even if they have met the recency of practice requirements they should still consider if what they are doing is within their current scope of practice or whether they should be self-limiting themselves or engaging in further training, assessment, and oversight.
Scope of practice can be a bit difficult to define at times. The Medical Board of Australia defines it as follows:
Scope of practice means the professional role and services that an individual health practitioner is trained, qualified and competent to perform.
Medical Board Australia
Most specialty colleges, for example, will have a statement on their website in relation to the type of clinical practice that they consider a Fellow of the college can safely engage in as a current Fellow of that college.
If you are working as an International Medical Graduate in Australia you may have some limits on your (scope of) practice imposed as part of your registration by the Medical Board. Typically these may be about only working in a particular area of medicine or only working in certain locations where supervision has been approved.
How do you prove recency of practice with the Medical Board of Australia?
Primarily and initially it’s an honesty system. Whenever you apply for registration or a new form of registration or apply to re-register you must indicate to the Medical Board that you meet the recency of practice standard.
The Medical Board does, however, expect that you keep a record of evidence to prove your recency of practice. And also indicates that it does from time to time audit for compliance and will look into your recency of practice further if it receives a notification about you.
What can happen if I give the wrong information to the Medical Board about my recency of practice?
In confirming your recency of practice you are confirming that you comply with the law. Deliberately lying about your recency of practice therefore can have serious consequences if you are found out. Even if you were not deliberately attempting to lie about your recency of practice if it turns out that you were non-compliant you could be in trouble.
What happens to my registration if I am not recent enough in my practice?
If you don’t meet the recency of practice standard then the Board can impose conditions on your registration or refuse your registration.
It is up to you to provide information to the Medical Board to help it decide whether you can safely continue with your registration.
Requirements for medical practitioners with non-practising registration or medical practitioners who are not registered and wish to return to practice (includes international medical graduates).
Have had 2 or more years of clinical experience
Not practising for up to 12 months
No additional requirements to be met
Have had 2 or more years of clinical experience
Not practising for between 12 months and 3 years
Before re-commencing must complete the equivalent of 1 year’s relevant CPD
Have had 2 or more years of clinical experience
Not practising for more than 3 years
Need to provide a plan for professional development and re-entry into practice
Have had less than 2 years of clinical experience
Not practising for more than 12 months
Required to recommence in a supervised training position
C/- Medical Board of Australia REGISTRATION STANDARD: Recency of practice 1 October 2016
For those doctors who are required to catch up with Continuing Professional Development the easiest path for doing this is via a college CPD program if you are a member of such a college. Many IMGs will register with the RACGP for this purpose, although it should be noted that RACPG CPD is technically only relevant to general practice and not hospital medicine, although clearly there is overlap.
If you have been out for more than 3 years and are a member of a college then you will normally find that the college provides a re-entry program option that will satisfy the Medical Board requirement. Generally, this will involve working under the oversight of a college fellow for a period of time.
What if I am changing scope of practice?
Again according to the Medical Board, if you are changing your field or scope of practice, you may need to undertake further training to ensure your competency.
If the change is to a subset of your current practice, i.e. you are narrowing your current practice, there are no additional requirements.
If you are changing your practice in a way that your peers might view as requiring you to undertake more training or you are changing to an entirely different field of practice then you will be required by the Medical Board to consult with the relevant specialist college to develop a professional development plan before entering the new field of practice.
Why do employers have a different interpretation of recency of practice?
Employers are of course obliged to take the Medical Board recency of practice standards into account when considering applicants for job positions. However, employers can and often do make their own interpretations around recency of practice.
Because working supervised is an option for addressing issues around recency of practice employers may consider doctors for posts where the doctors have been out of practice for significant periods.
However, it is my experience, particularly when it comes to trainee positions and international medical graduates that employers are unlikely to see large gaps in clinical practice favourably. Employers usually have several applications to consider and they will tend to take the easier path of employing a doctor who is either just moving between jobs or has 2 years or less time out of medicine.
What are the options for addressing recency of medical practice?
Option 1. Work under supervision to obtain recency of practice
As the Medical Board itself indicates if you have recency of practice issue then working under supervision is an option for addressing this matter. A key point of this standard is to ensure that doctors who are not recent enough in their practice are given some oversight to return to work.
So in theory this means that if you are applying for a resident or registrar (trainee) role recency of practice should not really be an issue from a registration standpoint. But as we have highlighted above it may cause a problem in terms of your candidacy versus other candidates who do have recency of practice.
Option 2. Gain some clinical experience elsewhere to gain recency of practice
If working under supervision in Australia is not really an option for you then your next option is to regain clinical experience by working in another country. The Medical Board indicates that it considers clinical practice in overseas countries as meeting the standard of recency of practice.
This is generally an option for most IMGs and something I tend to recommend if they have been more than 2 years away from clinical medicine.
I will generally advise that you try to work for 3 months back in your own country, or another country where you have a registration, as this will then help you to both meet the Medical Board’s recency of practice standard as well as provide some reassurance to employers.
Are courses and observerships useful for recency of medical practice?
In a couple of words not really. Neither really helps that much.
Certainly, from a Medical Board perspective, observerships do not count as clinical practice towards the recency of practice requirement. Courses may be of assistance if you are required to undertake CPD relevant to your scope of practice.
From an employer’s perspective, a relevant course might help a fractional amount and an observership may also assist in a small way. The key benefit for an observership may be in being able to nominate a referee who has recent contact with you in the Australian health context. However, the merits of an observership are marginal compared to actual clinical practice.
Disclaimer. This post was written having researched the current standards for recency of practice. You should always consult an expert to gain individual advice on your circumstances, check out the official advice, and be mindful that guidelines and policies do change over time.
Related Questions.
Who Does Recency of Practice Apply to?
The recency of practice registration standard applies to all registered medical practitioners, except those with non-practising registration and recent graduates applying for provisional registration to undertake an accredited intern position.
Who Does Recency of Practice Not Apply to?
Recency of practice does not apply to non-practising clinicians or interns provisionally registered. It also does not apply to registered students.
Does Recency of Practice Only Affect International Medical Graduates?
No. The recency of practice standard affects all medical practitioners seeking registration or re-registration in Australia, including locally trained doctors.
What is Meant by Scope of Practice?
Scope of practice generally refers to the areas of medicine you are deemed fit to practice within.
If I Work More Than 38 Hours in a Week. Can I count These Additional Hours Towards Demonstrating Recency of Practice?
No. You may only accumulate 38 hours in one week. Additional time will not count towards the standard.
What If I Work Part-Time?
Doctors who work part-time must still complete the same minimum number of hours of practice – this can obviously be completed part-time over more weeks, for e.g. working 20 hours per week for 8 weeks of the year would meet the standard.
Will Doing a Certain Course Help My Recency of Practice?
From a Medical Board perspective courses and degrees do not assist in any way with the recent of practice standard. From an employer perspective, they might assist in a very marginal way but really nothing beats recent clinical practice.
Will Doing an Observership Help My Recency of Practice?
From a Medical Board perspective, observerships do not count as clinical practice towards recent of practice. From an employer perspective, an observership may assist in a small way. The key benefit may be in being able to nominate a referee who has recent contact with you in the Australian health context. However, the merits of an observership are marginal compared to actual clinical practice.
Does Overseas Experience Count?
Absolutely. The Medical Board “accepts practice outside Australia for the purposes of meeting the recency of practice registration standard.”
For psychiatrists, Australia presents excellent job prospects. And it really has been this way for a long, long time. As a Fellow of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) you can literally work anywhere in Australia and pretty much in any particular field, whether that be general psychiatry or something specific like a child and adolescent psychiatry or working in public or private or even both. Having spent a fair amount of my career filling positions in psychiatry I wanted to share my experience and advice with you.
In answer to the key question. How does one become a psychiatrist in Australia? Well, to work as a psychiatrist in Australia, you must obtain a Fellowship of the Royal Australian and New Zealand College of Psychiatrists (the RANZCP). For locally-trained doctors, this involves completing a medical degree, at least one yearinternship, and a minimum of 5 years of training with the RANZCP. For specialist international medical graduates (IMGs) you must apply to the RANZCP for specialist recognition of your overseas training and experience.
Let’s look at psychiatry careers now in a bit more depth.
There are lots of job vacancies for both local as well as overseas trained psychiatrists in Australia.
There are lots of job vacancies for Psychiatrists in Australia (as there is in most other parts of the world). Mental health is a growth area, although arguably it’s more accurate to say that we are just now realizing how important it is relative to somatic medicine.
This all makes the task of those recruiting to Psychiatry positions tricky. I have had personal experience with this in past roles and have been quite successful in managing to put together strategies to fill positions. In Australia, it is quite common for recruiters to have a strategy of filling positions from international medical graduates (IMGs).
If you are an IMG Psychiatrist or even an IMG trainee in some cases. Then you will find that there are plenty of opportunities available to you in Australia. In fact, psychiatry is possibly the most accessible medical specialty for IMGs to access in this country.
In this blog post, I wanted to share my experience with you and highlight some tips. Here’s a summary of what we will discuss about the prospects of IMG doctors working in psychiatry in Australia:
There are a number of vacant psychiatry consultant positions as well as vacant psychiatry trainee posts all year round in Australia.
Unlike the specialist pathway for most other specialties, if you are an IMG psychiatrist you must have a job offer first before the RANZCP will consider your application, this is a good thing.
The majority of specialist psychiatrists from Competent Authority countries will likely be found to have substantial comparability and specialist psychiatrists from other countries are likely to be found partially comparability although substantially comparable is not out of the question.
If you are a trainee psychiatrist from the United Kingdom, Rep Ireland, Canada or the United States you will easily find a spare training post to fill under the competent authority pathway process.
Whilst the prospects are very good you do need to be sincere, prepared to do some work to make yourself an attractive candidate and be prepared to be a little bit flexible, particularly in where you might work for your first job.
If you are excited so far then you may wish to fill out the quick survey below where we can provide you with an immediate quick appraisal of your prospects, as well as review your career profile in more depth for you.
Take Our Survey and See If you Qualify for a Free Call
[fluentform id=”9″]
With that synopsis out of the way let’s dive further into the detail.
What does a psychiatrist do in Australia?
According to the RANZCP a psychiatrist, you will be able to:
listen to and provide expert care for vulnerable people and their families and work to prevent, diagnose and treat mental health conditions, lead teams of other doctors and health professionals, research to lead breakthroughs in psychiatry and mental health, foster new generations of psychiatrists, provide expert opinion to the community, government and courts.
How do Australian doctors become psychiatrists?
For an Australian doctor to become a psychiatrist they need to:
complete a medical degree
do on-the-job training in a hospital for at least 12 months, i.e. complete an internship
enrol and complete training in the medical specialty of psychiatry with RANZCP.
Specialty training is a minimum of 5 years and leads to the Fellowship of RANZCP, the FRANZCP. Whilst the RANZCP still views the FRANZCP as a generalist qualification there are a number of Advanced Training programs or certificates that you can undertake to extend your knowledge in certain aspects of psychiatry, including child and adolescent, consultation-liaison, psychotherapy, forensics, old age to name a few.
How do overseas training programs align with the RANZCP?
Because being a psychiatrist is still considered to be mainly a generalist role in Australia most overseas specialty programs will align well with the RANZCP because these are also fairly generalist in their approach in the main as well.
There are sometimes some exceptions. For example, in the United States, it is possible to train primarily as a child and adolescent psychiatrist with little or no adult experience.
And occasionally when IMG psychiatrists apply to the RANZCP they are found to be a bit lacking in certain experiences that are a requirement here in Australia. Again, the most notable is the requirement to do at least 6 months of child and adolescent psychiatry training. This is however rarely a deal-breaker and usually only results in an extra recommendation of some additional time in child and adolescent psychiatry as part of the supervised component of the specialist pathway.
What are the chances of getting a job as a Psychiatrist in Australia?
Again, according to the RANZCP:
The likelihood of finding a job as a psychiatrist is very high. There are not enough psychiatrists to meet demand, especially in rural areas.
ranzcp.org
In fact you don’t really even need to look at rural areas of Australia. As you can see by this recent shot from one medical recruitment company website.
As you can see from above there are both consultant (Staff Specialist) roles available as well as trainee roles (Registrar) in major capital cities such as Perth and Canberra and regional coastal areas.
What can you earn working in Psychiatry in Australia?
The above image also gives you an indication of the salary packages, which for Consultant Psychiatrists range from $300K to the high $400K.
Sometimes specific additional incentives are applicable for psychiatrists and I was recently successful in obtaining a package of almost $500K for a particular psychiatrist. This is one of the reasons why being open to working in regional areas may make sense as your package may be better and generally your standard of living (particularly housing costs) will be much lower.
On top of the package for IMG Psychiatrists, employers are often also prepared to help with moving costs and may also pay for the cost of applying to the RANZCP from your professional development fund.
Whilst the pay packets for trainee psychiatry doctors are obviously not nearly as large as for consultants, you may still earn a bit more than the annual salary through performing overtime shifts (which are generally paid at 2x the hourly rate) and it is not unheard of employers also offering to cover some moving costs for trainee doctors as well.
What qualifications do you need to work in a Psychiatry job in Australia?
Your qualifications will be assessed by the RANZCP. In general, you will need some form of postgraduate qualification that is preferably at least 4 years duration.
For the UK/Ireland – MRCPsych combined with the CCT in the UK or CSCST for Ireland.
For Canada, you will require a Certificate in Psychiatry from the Royal College of Physicians and Surgeons of Canada.
For the USA, you will require a Certificate of the American Board of Psychiatry and Neurology.
For India, you will need a minimum of an MD or equivalent in Psychiatry, preferably you will do more than 3 years training. The addition of the Diplomate of the National Board is generally seen as a good addition.
For Sri Lanka, you will need a minimum of MD in Psychiatry recognised through the Postgraduate Institute of Medicine and be board certified as a psychiatrist via the Sri Lankan Medical Council.
What is the process for obtaining specialist recognition as a Psychiatrist in Australia?
The process is the same as for other specialist IMGs. Your educational qualifications and training as well as your specialist practice will be assessed by the RANZCP for comparability.
If you are deemed to be within 12 months of becoming a psychiatrist, you will be offered substantial comparability, which is the best outcome as this generally requires you to work as a specialist under peer review by current Fellows of the RANZCP for 12 months.
If you are deemed to be within 24 months of becoming a psychiatrist, you will be offered partial comparability. This is the next best outcome and generally requires you to work in an appropriate Advanced Trainee position, as well as under peer review by current RANZCP Fellows. It will also require you to undertake a range of assessments and activities as well as sit for written and clinical examinations.
If you are not deemed to be able to become a psychiatrist within 24 months you will be found not comparable. This means that you need to consider alternative pathways for registration and working in Australia.
from RANZCP SIMG Assessment Form
One key difference from the process of specialist assessment for other colleges is that the RANZCP requires you to have an offer of an appropriate position first before considering your specialist pathway application.
Whilst this may seem initially restrictive it is probably better. Because it reduces the number of specialist IMGs who are deemed comparable but are unable to gain an appropriate job offer. It also means that you are more likely to be supported by your employer to go through the RANZCP assessment process.
Whilst it is not absolutely guaranteed. Being interviewed successfully for a position as a psychiatrist in Australia will generally mean that the RANZCP will also find you comparable.
What types of comparability outcomes are likely for international psychiatrists in Australia?
As can be seen in the images below taken from the most recent Medical Board of Australia report the majority of specialist IMG applications to the RANZCP are deemed substantially comparable with a significant number deemed partially comparable and only a small number seen as not comparable.
Outcome of interim assessment 2019 by college.
Does your country of training have any impact on your prospects for psychiatry jobs in Australia?
Whilst we don’t have figures by country of IMG versus the RANZCP assessment process it’s my experience that specialist psychiatrists from the competent authority countries are generally found to be substantially comparable. Specialist psychiatrists from other countries are more likely to be found substantially comparable, however, it depends on your individual circumstances and it is not uncommon for specialist psychiatrists from India, Sri Lanka, and South Africa to be found substantially comparable at times.
Empirical evidence for this exists when you look at the overall comparison between specialists from India and the UK in the same report.
Outcome of Interim Assessment 2019 by country.
What do you need to demonstrate if you want to work as a Psychiatry Trainee in Australia?
In order to convince an employer that you are suitable to work in a trainee psychiatry role you generally need some prior psychiatry trainee experience in your own country.
Because the process of becoming registered under the competent authority pathway is more streamlined and because the training programs in the competent authority countries are similar to that in Australia, trainee doctors with psychiatry experience in the UK, Ireland, Canada, or the US tend to be preferred by Australian employers when it comes to filling vacant trainee positions that have not been able to be filled by local graduates.
Whilst it is not impossible for trainee psychiatry doctors from other countries to also obtain posts it is more difficult as the process of gaining registration is more complex. If you have significant experience as a trainee psychiatrist, you may be able to obtain a position for a maximum of 2 years under the short-term specialist medical training pathway.
Is there recognition of prior learning for IMG trainees?
Colleges have become better at assessing trainee doctors from other countries for recognition of prior learning (RPL). In fact, I recently assisted a trainee doctor from the UK to obtain 2 years and 7 months from their 5-year RANZCP psychiatry training program.
That being said RPL generally reduces the amount of experience you may have to undertake and doesn’t normally excuse you from the key RANZCP examinations. The end effect may be to compact the number of assessment requirements you need to complete in the remaining time.
Take Our Survey and See If you Qualify for a Free Call
[fluentform id=”9″]
Some Tips For Securing A Psychiatry Post In Australia.
Thus far it probably sounds like being able to work as a psychiatrist in Australia is a bit of a laydown misere. And whilst it is true that psychiatry is one of the top medical specialties that employers are regularly trying to fill in Australia. It is not just a matter of sending off a quick email with a CV that hasn’t been updated in a few years. There is still a bit of work ahead of you.
Here are my recommendations for what you should do if you are keen on working in psychiatry in Australia.
First off, ensure that you have an up to date and employer-friendly resume. This should be around 3 to 6 pages depending on your experience. And you should make sure wherever possible you tailor it to individual job openings. If you are needing tips on your resume (CV) we have several posts about this matter on the blog, as well as a service for helping you redo your resume if you would like some assistance with this key document.
Second, if you are going to apply for a specialist role it’s worth reviewing the documentation on the RANZCP website to see if you will be eligible. And we also have a handy free short course on the specialist pathway that you can take as well.
Third, whilst it is sometimes possible to score a post in a major Australian city like Sydney or Melbourne. If you are too prescriptive about where you want to work you are very likely to severely limit your chances and miss out. Bear in mind that once you complete your first year or two under supervision you will normally then be eligible for either specialist registration or general registration. At this point, you can often move jobs and locations more easily. So the key message here is to be open to all possibilities for your first position. You may even like working in regional Western Australia or the North West Coast of Tasmania!
Fourthly. And following on from the above point. Whilst it is possible to directly approach employers for posts in psychiatry. This is only really about 50% of the job market. It is often unclear which publicly advertised positions are open to IMG doctors and employers are also often directly working with medical recruitment companies to fill vacant spots. For this reason, I generally recommend that you do contact a medical recruitment company if you believe you are eligible for a specialist position as an IMG or a trainee psychiatry doctor from one of the competent authority countries. If you fill in the survey below we can put you in contact with our recommended medical recruitment company.
Fifth and finally. If an employer is interested in you they will invite you for an interview. This may be the first time you have sat a job interview in sometime and will almost certainly be the first job interview you have sat in Australia. You may be a little nervous and it will be important to give an impression. You may therefore want to consider getting some assistance by way of some interview coaching beforehand.
Related Questions
Can overseas doctors work as a psychiatrist in Australia?
Yes. There are lots of opportunities and vacant positions for suitably qualified psychiatrists from other countries (IMGs) to work in psychiatry jobs in Australia. There are also numerous openings for appropriately experienced psychiatry trainees.
What qualifications do you need to become a psychiatrist in Australia?
To become a psychiatrist you need to: 1. complete a medical degree. 2. do on-the-job training in a hospital for at least 12 months (internship). 3.enrol and complete training in the medical specialty of psychiatry with RANZCP. Qualified psychiatrists from other countries apply to the RANZCP for assessment of their specialist recognition under the specialist pathway for medical registration.
How much does a consultant psychiatrist earn in Australia?
As we have highlighted in this article for a permanent full time public health service position you can be expecting to earn around $350,000AUD to $450,000AUD per annum. Psychiatrists also do relatively well in the private sector and you can potentially earn far more than in the public sector and up to $800,000AUD. As we have highlighted in this related blog post, psychiatrists are 5th on the list of top ten professions by earnings according to the Australian Tax Office.
How long does it take to become a psychiatrist in Australia?
To become a psychiatrist you: study medicine and complete a medical degree (4-6 years) do on the job training in a hospital after your degree (1 year) enrol and complete specialist training in psychiatry (5 years) with RANZCP. So all up its at least 10 years, generally longer.
What field of psychiatry makes the most money?
As is generally the case with other medical specialties, consultant psychiatrists will make significantly more money than other health professionals working in the mental health field, e.g. psychiatry trainees, psychologists, social workers and nurses. It’s hard to say which actual field of psychiatry makes the most money. There are certain subspecialties in psychiatry that are more limited to working in public hospital settings, for e.g. consultation-liaison psychiatry, so these consultants will earn a bit less than someone working in the private sector. Subspecialties that lend themselves best to private sector work, and which will therefore, have higher earning potentials, including forensic psychiatry and adult psychiatry.
*The process of getting a job and getting registered as a doctor in Australia is complex, it’s important to understand that you do need to get individual advice on your circumstance. Circumstances do vary for individuals and also things change over time.
If you are an ad doctor looking for some general information about your options for getting registered in Australia, then this post is for you. I spend a lot of time on Zoom calls these days explaining to doctors from overseas countries (International Medical Graduates or IMGs) what their options are for working as a doctor in Australia. It’s quite a complex process. And inevitably at some point, it makes sense to talk one on one. Particularly if you are starting to get serious about the idea of working as a doctor in Australia. If that’s you I’d recommend booking a strategy call.
With that being said. Let’s look at the four pathways available for IMG doctors to become registered in Australia from overseas. And let me be quite clear here. These are not the main pathways. They are the only pathways available for getting registered in Australia, at the time of writing this post. If you are a doctor coming from overseas to Australia your pathways to registration are:
The Standard Pathway, which is a general registration pathway for doctors from any country who do not have specialist qualifications and are looking to start at junior doctor level in Australia.
The Competent Authority Pathway, which is a restricted pathway that enables both specialist and non-specialist doctors from the United Kingdom, United States of America, Republic of Ireland and Canada to commence their work in Australia.
The Specialist Pathway, which is a pathway that can ultimately lead to recognition as a specialist in Australia and requires you to be initially assessed by the relevant medical specialty college.
The Short Term Training in a Medical Specialty Pathway, which allows for time-limited registration, so that advanced trainees and specialists from other countries can obtain some top-up training in Australia.
It All Comes Down To the Medical Board of Australia.
So the first thing to know about getting registered in Australia is that it’s the same final authority wherever you work in the country. No matter what state or territory you are in, it’s all conducted through what’s called the Medical Board of Australia under the overarching umbrella of the Australian Health Practitioners Regulation Agency.
This is actually a reasonably new thing in Australia. Prior to 2010, the various state and territory medical boards were responsible for registration, which actually made the process even more complex.
Under the Medical Board of Australia, there are essentially four pathways to becoming registered as a doctor in the country. And if you’re an IMG, you can find some very helpful information about these pathways on the board website.
There are even handy flow charts that can help you make some decisions about which option might be best for you.
But It All Starts with the Australian Medical Council.
Whilst the endpoint for registration for IMGs is the Medical Board the starting point is always the Australian Medical Council. For some IMGs (those attempting the Standard Pathway) you will have a lot to do with the AMC. But for the rest it’s really a very quick but mandatory step where you have to get your medical degrees verified.
Why Have Pathways to Registration?
Pathways to registration in this country for international medical graduates are essentially comparisons against the process by which Australian and also New Zealand medical graduates are given registration.
Australian graduates first become registered in the system upon graduating from medical school as interns and progress through what is called provisional registration to general registration. After this most Australian doctors hope to eventually add what is called specialist registration to their registration status at some point.
The four pathways to getting registered in Australia are therefore pathways that lead to a form of initial or provisional registration. But which ultimately lead to the IMG being able to gain either general or specialist registration. This is with one notable exception. The Short Term Specialist Training Pathway, which is a time-limited pathway that does not lead to either general or specialist training.
The Competent Authority Pathway.
The competent authority (CA) pathway essentially recognises that doctors that come from other healthcare systems, with similar systems, and processes, and standards to the Australian context, have a level of equivalence.
The competent authority pathway is for both non-specialists as well as specialist doctors. It is a streamlined process for becoming granted registration in Australia. The board has approved a number of international authorities as competent in their assessment of doctors for medical registration. The reason that these authorities are deemed competent (and others are not) is unclear but historically well before the advent of the Medical Board of Australia, these jurisdictions were given preferred status by the old State and Territory Medical Boards. Arguably these countries do have medical training systems that are equivalent to Australia.
The authorities are:
the General Medical Council in the UK for local UK graduates as well as international graduates who go through the PLAB pathway.
the Medical Council of Canada.
the Educational Commission for Foreign Medical Graduates of the United States and the United States Medical Licensing Exam (essentially, anyone who has the USMLE certificate).
the Medical Council of Ireland.
And the Medical Council of New Zealand*
*The Medical Council of New Zealand is only listed here for IMG doctors who go through what’s called the NZREX process. Something akin to the AMC Standard Pathway process in Australia. Actual medical graduates of medical schools in New Zealand are considered absolutely equivalent to Australian graduates of Australian medical schools because these schools are actually also accredited by the Australian Medical Council.
So if you have primary qualifications in medicine awarded by a training institute, which is recognised in the competent authority jurisdictions and also recognised by the Australian Medical Council you will normally be permitted to apply to work as a doctor in Australia under this pathway.
This is on the proviso that you have completed some clinical training or assessment within that authority. This differs from jurisdiction to jurisdiction but is either a year of training or two. So, for example, in the UK, that would be the first foundation years. Whereas in the US it would mean completing 2 residency years in an ACGME accredited post.
Why Is The Competent Authority Pathway Attractive?
If you are eligible for the Competent Authority Pathway in Australia this is generally a good thing as it is considered to be the easiest pathway to getting registered and being able to start working here.
Often times employers will also prefer say a UK-trained doctor over a doctor from Sri Lanka when there is a need to employ an IMGs.
If you are eligible for the Competent Authority pathway essentially all you need to do is convince an employer to offer you a suitable position and have the intended supervision for this position assessed by the Medical Board of Australia.
Once you are approved for registration you work for 12 months under provisional registration and will need to complete satisfactory supervisor reports. If all goes well at the end of this process you are able to apply for general registration. There’s no need for examinations or other forms of assessment (other than supervisor reports).
(It should be noted that sometimes doctors from CA countries who are applying for specialist registration also work for 12 months under this pathway. In this situation you do not gain general registration at the end of the process you gain specialist registration in your particular specialty.)
The Standard Pathway.
The next pathway is the most common pathway that the majority of IMGs attempt in order to work as doctors in Australia.
The standard pathway applies to IMGs who are not eligible for the competent authority pathway and who do not have specialist qualifications. To come in through this category, you need to have a recognised primary qualification in medicine. But before you can apply to the Medical Board of Australia for registration or approach employers for jobs, you have to go through some additional steps with the Australian Medical Council.
These steps include the mandatory check of your degree, which all IMGs have to do. But also include sitting for the AMC Certificate examinations, which is a 2 part examination, consisting of a Part 1 MCQ Exam, and then a Part 2 Clinical Examination.
You can actually begin to apply for jobs once you have successfully passed the AMC Part 1. But you will only be able to gain general registration once you have completed the full certificate.
We have a guide to the AMC exam here. The AMC Exam, particularly the clinical exam, is generally considered to be a very tough and difficult examination to complete. Despite this, there are quite a few IMG doctors who have obtained their certificate but have been unable to find employment as a doctor in Australia.
The Specialist Pathway.
The final main pathway for most IMGs is the specialist pathway. This pathway is for overseas trained specialists so that they can apply to be assessed against the capability of a similar Australian-trained specialist. A process that is called “comparability”.
This process includes IMGs applying for what is called Area of Need positions, which are extremely rare to find these days. As well as specialist IMGs just going for assessment with the college.
As with all other pathways, you need to have a recognised primary degree first. But then just to create more confusion IMGs applying for the specialist pathway don’t apply to the AMC or the Medical Board for assessment they apply to the relevant specialist college. Which then performs an assessment.
So if, for example, you’re a specialist from a competent authority country, it can be very confusing because you can apply to the Medical Board of Australia for provisional registration under the competent authority pathway to work in a supervised position.
But at the same time, you need to also apply it to the college to assess your specialty training and experience and qualifications in order to get registered as a specialist and come through the specialist pathway.
Applying for the Specialist Pathway assessment involves quite a bit of time and money. In general, you will need to fill out an extensive application outlining all of your past experiences to date. The more complete and detailed you make this generally the better the outcome. The college may just reject you based on your application. But generally, in the case of most colleges you are then invited to an interview to further explore your credentials.
There are only 3 outcomes for this assessment process:
You are deemed not comparable.
You are deemed partially comparable.
You are deemed substantially comparable.
Being deemed not comparable means you need to think about other pathways.
Being deemed partially comparable or substantially comparable means that the college views you as either being within 2 years (partially comparable) or 1 year (substantially comparable) of becoming a specialist in Australia.
If you achieve comparability you will still need to secure an appropriate post where you can receive oversight by other specialists in your field. In the case of partially comparable, it is also likely that you will need to sit further examinations.
If you gain a post and complete all the requirements you will finally be recommended to the Medical Board for specialist registration.
We will eventually have a more detailed post about the specialist pathway. But in the meantime the following 2 blog posts are useful:
As well as our series of videos on the Specialist Pathway on YouTube.
The Short Term Specialist Training Pathway. The Final Pathway.
There is actually a fourth pathway option. This option is not as well known to IMGs as the other 3 options. And this is perhaps because it is not a pathway to permanent registration in Australia.
The final pathway is called the Short Term Training in a Medical Specialty Pathway, or Short Term Specialist Training Pathway. This pathway is limited to IMG doctors who are either already specialists or in the advanced or final phase of their specialty training. Ostensibly the pathway is designed to facilitate additional “top-up” training or experience, i.e. it is designed to give a specialist from another country some additional training and experience to help when they return to their own country.
The pathway is therefore strictly limited to 2 years and you generally have to complete a form indicating that you are intending to return to your own country at the end of this period of registration.
To be eligible for this pathway you first need to secure a job offer (usually an Advanced Training post) from an employer. Like all other pathways, you need to verify your degree with the AMC. You also need to apply to the specialist college for assessment of your credentials against the post you have secured.
Unlike the specialist pathway, the college assessment is only paper-based, requires less information, and generally easier to pass.
Is Short Term Specialist Training A Pathway to Working Permanently in Australia?
Even prior to the advent of the one Medical Board there were registration categories in existence that enabled trainee doctors from other countries to come to Australia and work for a limited period of time.
It was not uncommon for these doctors to take the opportunity whilst working in Australia to pursue other forms of registration and the case is the same still with the Short Term Specialist Training Pathway.
So, whilst the pathway itself is designed to be time-limited and there is a requirement to state your intention to return at the end of your registration period. There is really no way of enforcing this and there is nothing to say that you might change your mind halfway through the process.
And I have certainly seen a number of IMG doctors use this particular pathway as a “stepping stone” to a more permanent registration category.
Whilst, specialist colleges are not permitted to take into account any experience you have gathered under the Short Term Specialist Training Pathway, it is hard for them to ignore the fact that you have already worked successfully in the Australian context and also hard to ignore references from Australian College Fellows attesting to your capability.
Similarly, if you have proven your work capability in an Australian health service then this tends to dramatically improve your prospects with employers in Australia for other jobs over and above most other things, including things like qualifications and observerships.
Related Questions.
I Have More Questions About the Standard Pathway and AMC Exams.
We recommend you check out this extensive post that we wrote.
Where Can I Find More Information About the Specialist Colleges?
Unless you have high schooled and trained in English in a small number of countries that the Medical Board recognises it is likely that you will have to pass one of the English competency tests. This is a requirement prior to obtaining registration and may also be required prior to other assessments, such as specialty college assessments. We have a detailed guide about this issue here.
One of the most frequent questions I receive from doctors from overseas is “How do I get into residency training in Australia?” Becoming a specialist doctor is generally a very rewarding pathway, which can afford a lot of independence and financial stability and is probably the ultimate aim of most doctors in Australia
So I have put this post together as an overview of how this all works. In so doing I wanted to make a few key points:
1. The process of becoming a specialist doctor in Australia is termed “specialty training” and in most cases is conducted via one of the 16 specialist medical colleges.
2. Residency training, which is often what doctors from places such as North American and Asian countries refer to when they are talking about specialty training, does not exist as a concept in Australia. And in fact, being a “resident medical officer” means something quite different here.
3. There are around 64 different medical specialties to choose from in Australia, and this includes general practice, which is recognised as a specialty in its own right.
How and when do local graduates enter into specialty training?
Medical school has been rapidly evolving in Australia of late with the majority of schools phasing out the old MB BS programs in favour of 4 or 5 year MDs. Some of these are graduate programs. So its not surprising to hear that for some the process of choosing and targeting a particular specialty begins early in medical school.
However, unlike say the North American system you can’t simply apply for specialty training at the end of your medical school.
Upon graduating there is a requirement for a minimum of one year supervised training which is referred to as an “internship”. It is only after you satisfactorily complete your internship that you gain general registration. Doctors from the United Kingdom and the Republic of Ireland would be familiar with something similar. The Australian medical training system has largely been adapted from the UK system.
The internship period is heavily supervised and there are a formal training and assessment processes, with oversight provided by bodies in each State and Territory called Prevocational Medical Councils.
This prevocational period often extends for at least another year and we call it prevocational training.
Resident Means Something Different in Australia.
A Resident or Resident Medical Officer, or RMO in Australia is a doctor in their second year out of medical school, i.e. someone who has completed their internship.
Whilst it is technically possible to enter into some specialty training programs as a Resident (Psychiatry and General Practice being examples) generally most doctors wait until the end of their second year to enter into training. And in the case of some particularly competitive specialties, such as surgical specialties and anaesthesia, may wait several more years to get on to a training scheme.
A doctor who is still a resident in their third year is generally referred to as a Senior Resident.
For most senior resident doctors, there is no set standard or oversight for training. So the quality of support provided can vary quite considerably. And it can often be left up to the individual to develop their own program. This situation has unfortunately led to some fairly famous recent cases of exploitation of doctors working what are termed “unaccredited posts”. These are posts that are not oversighted as an official training post by a college. Often referred also to as service roles.
It’s for this reason that doctors in Australia are often relieved when they finally make it into a specialty.
For International Medical Graduates coming via the standard pathway or in some cases also the competent authority pathway. Its a Resident post that you are looking to fill as your first job in Medicine in Australia, i.e. a pre-specialty training position.
Key Requirements for Specialty Training.
The requirements for entry into specialty training differ between colleges and this post is not intended to address each one specifically. But let’s look at some of the general requirements.
You Must Have General Registration to Enter Specialty Training.
One thing that every doctor must have to enter into specialty training in Australia is general registration. So for local graduates, this means completing an internship first. For IMGs this means completing a provisional year, normally as a resident, either via the standard pathway or competent authority pathway, after which you will also be granted general registration.
This is why I often tell IMG candidates that once you have completed your supervised year you are almost on an equal footing with local graduates.
You Generally Need at Least 2 Year’s Experience.
Most but not all colleges require you to have gained a minimum amount of clinical experience prior to applying. The most common requirement is for 2 years.
Whether this is a valid requirement or not is somewhat questionable. As noted some colleges now allow doctors to apply after completing an internship.
A key driver for maintaining a second-year residency in Australia is the need for doctors to fill service level roles. But to be fair many doctors themselves also value having 2 years to consolidate after medical school.
Having Permanent Residency Or Citizenship Can Also Be A Requirement.
In some cases, for example, the Royal Australasian College of Surgeons, you will also need to prove that you are a Citizen or permanent resident. So this can be a discriminator against IMG doctors.
I am often asked why there is this discrimination in place. To be fair to the colleges they are really only applying the Australian law which essentially dictates that jobs must be provided to citizens and residents first before being offered to someone on a visa. Many other countries have similar arrangements for their own citizens.
The Application Process Itself.
The application process itself is similar to a normal job recruitment process. There are 2 main ways to get selected into specialty training in Australia.
1. College Goes First.
The first way is to get selected by the College first. This is the approach that most Colleges adopt. Examples, include RACS, RANZCO, RANZCOG and RANZCP.
For trainee doctors, this selection process may be the most rigorous job interview that they ever encounter, with many colleges employing scoring criteria for both your CV, as well as referees and submitting candidates to psychometric testing and a multiple mini interview approach.
There is often a fee of several thousand dollars to apply with no refund if you don’t make it!
After the college has selected which candidates it prefers for training the employers (the hospitals) may invoke their own second selection process or just accept the finding of the college.
2. Employer Goes First (Alone).
If you are applying for Physician training or Radiology training then you will start off by interviewing for a training post which is held by a hospital or health services. This will generally be a more standard affair, with an online application, CV and referee checks and interviews. Normally its just a panel interview but there has been a trend lately to making some of these recruitments multiple mini interviews.
There will generally be representatives of the respective college on the selection panel.
Once you have gained a post you will apply to be recognised as a trainee by the relevant college. In the case of Physicians, you can even do this beforehand. The process is generally just an application and fee and rarely are doctors rejected.
General Practice Selection.
General Practice Selection is a whole beast to itself, with many pathways.
The main pathway into GP training is conducted by the regional training providers, which are separate from the GP colleges. Selection is quite rigorous and also involves both psychometric testing as well as formal interviewing. Once selected, candidates then apply for one or both other College training programs for which they have already been deemed eligible bypassing the training selection process.
What Specialties Can You Apply For?
If we take the latest view from the Medical Board of Australia there are 64 recognised specialties for medicine in Australia. And below that many hospitals and employers will recognise even more subspecialties.
That seems a lot of choices. But actually the initial choice is made a little bit easier by virtue of the fact that many specialties break their training up into Basic and Advanced Training. Basic Training is usually around 2 or 3 years and more generalised. Once you complete Basic Training you can specialise further in Advanced Training. Which usually requires you to undertake an additional selection step.
Let’s look at some of the more popular specialty choices in Australia.
For General Practice. As indicated there are a number of pathways but the main pathway is the Australian General Practice Training Program under which you train for a Fellowship with either the Royal Australian College of General Practitioners or Australian College of Rural Remote Medicine.
For both Adult Medicine and Paediatrics you commence Basic Training with the Royal Australasian College of Physicians. After which you can choose to stay general in your Advanced Training or do one of many different specialties. The RACP also looks after some other smaller training programs, including Occupational Health and Rehabilitation Medicine.
For Radiology, you apply to the Royal Australian and New Zealand College of Radiology. This is a relatively straight forward specialty. There are really only two options. Diagnostic Radiology and Radiotherapy.
For Psychiatry, you apply to the Royal Australian and New Zealand College of Psychiatrists.
For Emergency Medicine, it’s the Australasian College for Emergency Medicine.
Surgery is a little different. Because its such a competitive specialty trainees have generally completed a lot of experience and courses just to get in. So you apply directly for “SET” (Surgical Education Training) in either of General, Vascular, Orthopaedics, Ear Nose and Throat, Paediatrics, Cardiothoracic, Neurosurgery, Urology or Plastic Surgery.
We have a more detailed post about the Specialty Colleges here.
Other Related Questions.
How Long Does Specialty Training Run For?
Answer. Most training programs are around 5 or 6 years minimum. Although General Practice can be as little as 3 years.
Do You Get Paid When Training?
Answer. It’s surprising how often this question is asked. And I guess it must be because in many countries you have to pay for a specialty training post or residency position. If you are employed as a doctor in Australia you are paid. This includes training roles. The salaries are pretty good although the work can be quite long in some cases. We have a salary guide here.
How Do You Enter Training Via the Competent Authority Pathway?
Answer. First of all. Like any other IMG you will need to get your credentials reviewed by the Australian Medical Council and then gain an appropriate job offer which permits you to have provisional registration with the Medical Board of Australia.
What post you are able to fill will largely depend on your current level of experience and training. If you have just finished Foundation Year in the UK then you will probably only be able to apply for Resident level jobs.
But let’s say you have almost finished your Residency in Anaesthetics in the US. Then you will probably be permitted to fill an unaccredited Anaesthetic Registrar post. But not something that you are not experienced in, such as a Psychiatry post. Once you have completed your 12 months supervision successfully you can apply for general registration, after which you can apply to enter training in Australia. You may be eligible for some recognition of prior learning.
How Do You Enter Training Via the Standard Pathway?
You must register with the Australian Medical Council and complete your AMC Certificate (Part 1 and 2). As well as obtain a post that allows you to work towards general registration. Its at this point that you can start applying for training posts.
Is There Some Recognition For Prior Learning?
Answer. In the past, it has been difficult to obtain much in the way of Recognition of Prior Learning from colleges but recently I was successful in helping one trainee doctor get almost 3 years credit for Psychiatry! Generally, you might expect to get one or two years off your basic training. Depending on how much training you have already done and how similar it is to training in Australia. Candidates from competent authority countries tend to do better with this process.
How Are Specialists From Overseas Treated?
Specialists from other countries can apply directly to the relevant college for an assessment of their capability to work as a specialist in Australia. This is known as the specialist pathway.
In this post, I want to go over a few of the common mistakes that I see specialists from other countries make when going through the process of applying to work via the specialist pathway in Australia. If you are reading this post. You are probably a specialist doctor in another country who is thinking about applying to work in Australia. Thanks for putting your trust in our blog. I have helped several doctors just like you to make this career move in the past.
I’d like to highlight that I now have a short course on the specialist pathway on my website that you can take for free that will help you to better assess your readiness to embark on this journey. There is a handy checklist in this course that will help you to make sure that this is the right option for your and if so that you are on track with your application and you don’t overlook a key element (such as the ones we have talked about already).
And a reminder that there may be other ways that I can help you out, including my RISK-FREE Strategy Call which is a great option if you just have a few questions or are struggling to know how to get started with the process.
In this post, I want to go over the 3 key mistakes that I see the majority of Specialist IMGs ignore to their detriment when attempting to work via the specialist pathway in Australia. These are mistakes that I see time after time. And the sad thing is that it is only often that someone comes to me late in the process to seek help on one of these problems. When, if they had come to me earlier or known about these issues, they could have saved themselves a lot of time, pain and heartache.
Specialist Pathway Mistake Number 1. English Language Proficiency.
So the first mistake often made with the specialist pathway is a pretty simple one. It’s not having the right English language proficiency. I’ve blogged and vlogged on this matter before. So I won’t give a detailed overview about English language proficiency in this post.
But suffice to say. An Australian specialty college is not going to assess you if you are required to prove your English Language proficiency.
Now if you are from a country where English is the main language, like the UK or Canada or the United States you are probably okay (BUT YOU SHOULD ALWAYS CHECK).
But if you are from most other countries such as India, for example, you will need to sit one of the four approved tests and achieve the required score.
It is vital that you do your very best on these tests by the way. As the level at which you score will affect whether employers are interested in interviewing you. With for example a candidate with an IELTS score of 8/9 being much more likely in my experience to score an interview than a candidate with the par score of 7/9. (All other things being equal).
If you haven’t sat your test and you apply to a college. Your application will be rejected until such time as you complete the proficiency test.
So this is a delay you can avoid.
I generally recommend preparing and sitting for your proficiency test whilst you pull together all the information required for your application.
Specialist Pathway Mistake Number 2. Not Reviewing Your Specialist Pathway Application Against the College Curricula.
In my experience, most Specialist IMGs (SIMGs) are able to navigate to the relevant college website and read through the relevant pages for IMGs, including finding the application guide and forms.
However, there are two things that most SIMGs do not look at on these websites, which are crucial to a successful application for the specialist pathway.
The first of these are the college’s relevant training curriculum
You see it is vitally important that you are able to demonstrate both in your application as well as your interview that your training and experience is as close as possible to what is expected of a specialist in Australia.
The best guide to this is what and how the college determines its own locally trainees should do.
As an example of this if you were applying to the Royal Australasian College of Physician as a General Physician you would be best advised to review your application against:
This document goes over in explicit detail what experiences and learning outcomes local physicians are meant to go through and how these are assessed.
This is by far the easiest way to work out how your training in your country stacks up against a specialist here and how to explain this training.
Most of these documents are publicly available. You just need to know where to find them. (See below). And they are normally very detailed. Often going for about 30 or 40 pages in length.
These documents can give you some hints about extra things you could do now to increase your chances for the specialist pathway. For example, perhaps there is a certain skill or procedure an Australia trainee is required to demonstrate. Maybe you can do a course on this skill or procedure or take a short post in a service in your own country that performs this skill or procedure?
Specialist Pathway Mistake Number 3. Not Reviewing Your Specialist Pathway Application Against the College Professional Frameworks.
The 3rd and last mistake when applying for the specialist pathway is similar to the previous one. That is not taking the time to find out about the Professional Framework for college Fellows in Australia.
Again. Most of these frameworks are easily found on college websites.
They give a guide to the types of behaviour and skills a consultant is expected to demonstrate and have and maintain in Australia.
Most of these are based upon the famous CanMEDS framework.
used with permission of RCPSC
If you are aware of these frameworks then you will be able to avoid a common error I see when reviewing applications for specialist assessment via the specialist pathway.
This mistake is to poorly describe your consultant experience in a narrow and clinical way.
Remember. The first thing that colleges tend to look at is the length and then the quality of your training.
If this is in any doubt (which it can often be). They want to then see that you are working in a consultant role in your own country, similar to how a consultant might work in Australia.
This not only involves demonstrating medical expertise at an independent level.
But also other things from these competency frameworks, such as managerial roles and quality improvement roles and of course teaching and supervision roles.
As a rule its important to document for every consultant job you have worked both:
The clinical responsibilities and achievements, including the level of autonomy you worked at (the colleges are generally looking to see that you were the most senior doctor responsible for your patients’ care)
As well as a broad range of other skills and achievements, such as teaching and training, performance managing other, being responsible for quality and safety, as well as research activities.
So these are the 3 key mistakes to avoid when applying for the specialist pathway in Australia.
Below for you is a handy overview of the colleges themselves.
A short list of the 16 Australian Specialist Medical Colleges (we include the College of Dental Surgeons here):
Read on further for more details about these colleges and what they do.
Now that you know what a specialty medical college is. Let’s talk more about some of the confusing points of colleges. What types of colleges there are in Australia and importantly how to work out which college is the right college for you.
The Status of the Specialty Medical Colleges in Australia.
In Australia the specialty medical colleges remain very powerful. With the possible exception of general practice (which is a specialty by the way) the specialist medical colleges generally have the oversight of and organize much of the specialty training that occurs in this country as well as continue to monitor the continuing professional development of their members (called Fellows).
What are the Medical Specialty Colleges in Australia?
Something that should be pointed out at this point is that most (but not all) of the specialty medical colleges in Australia are also the same college for the country of New Zealand. This has the handy advantage for Fellows of these particular colleges being able to be recognized and work in either jurisdiction. You will notice most colleges either refer to themselves and the “Australian and New Zealand College of”… or “Australasian College of”, for this reason.
See below for a full list of the current Medical Specialty Colleges in Australia along with links to their websites.
From each College home page there is usually an easily found link in the menu bar for prospective trainees, as well as international specialists looking for information about the specialist assessment process. We also have the direct links to the specialist assessment page here.
Our data sources for the table below come from the Colleges themselves as well as the latest available 2017 health workforce data, from the Federal Government. You can find the homepage for this data collection here.
Number of Fellows: 7661 Adult Medicine, 2258 Paediatrics* Main Post Nominals (FRACP).
*Actual total slightly higher due to other programs offered, some of which are jointly run with other colleges.
The RACP is one of the biggest Colleges. It also the most complex in terms of training programs. There are about 37 training programs. Fellowship of the RACP covers a range of aspects of specialty medical training, with a focus on Adult Medicine and Paediatrics.
If you are struggling to work out where your field of medicine fits, chances are it fits within the Physicians College. In the two main groups of Adult Medicine and Paediatrics and Child Health there are many subspecialties including General Medicine and General Paediatrics as well as things like Cardiology, Infectious Diseases, Geriatrics and Neonatal Care.
The RACP also covers 3 Chapter Training Programs in Addiction Medicine, Palliative Medicine as well as Sexual Health Medicine which you can enter after doing your Basic Training with the RACP or via training with another college.
Finally the RACP also provides 3 Faculty Training Programs in Public Health Medicine, Occupational and Environmental Medicine and Rehabilitation Medicine. Again, you can either enter into these after Basic Physician Training or by completing other prerequisites.
Fun Fact: The RACP even covers Dermatology for New Zealand!
Fellowship of the Royal Australasian College of Surgeons is one of the most highly sought after fellowships. Entry into any one of the 9 specialty training programs is highly competitive.
Number of Fellows: 40000+. Post Nominals (FRACGP).
The RACGP is by far and away the largest College in Australia. It is also one of the few colleges which does not have recognition in New Zealand.
General Practice is recognized as a specialty in Australia. In other countries this specialty may be referred to as Family Medicine, a Family Physician or Primary Care
Training to be a GP is conducted via a few different pathways. The largest one is the Australian General Practice Training Program, which is separate to the RACGP.
So the RACGP is a little different to other colleges in that, whilst it still sets training program requirements and conducts examinations, selection into training programs and training itself is done externally to the college.
The RACGP also provides an extension to its Fellowship where with a small amount of additional training you can be recognised as a rural GP (FARGP).
The RANZCP is one of the last true generalist specialist colleges in Australia. Its training program runs for 5 years and includes mandatory training in Adult Psychiatry, Consultation-Liaison Psychiatry (General Hospital Psychiatry), Child and Adolescent Psychiatry as well as a range of other types of experiences and assessments.
Towards the end of training, trainees can elect to undertake Advanced Training in a certain area of Psychiatry, including Child and Adolescent, Consultation-Liaision, Adult Psychiatry, Old Age Psychiatry, Neuropsychiatry, Forensic Psychiatry and Psychotherapy, however all trainees emerge from the program considered competent to work in all fields of the specialty.
It is expected that the position on generalism in Psychiatry will change in the not too distant future.
ANZCA ANZCA is responsible for the training, examination and specialist accreditation of anaesthetists and pain medicine specialists in Australia and New Zealand. In any given year there are about 1500 trainees undergoing training accredited by ANZCA in Australia and New Zealand. The College also has a number of trainees in Singapore, Malaysia and Hong Kong.
At 35 years ACEM is one of the newer colleges in Australia. It is also one of the first colleges in the world that represented the specialty of emergency medicine that emerged (pardon the pun) in the 1970s from hospital casualty department medicine.
The Association of Casualty Supervisors of Victorian Hospitals (ACSVH) was the first body in Australia to focus on Emergency Medicine. Its formation followed a 1973 report on the Royal Melbourne Hospital’s Casualty Department and observations of similar facilities in Western Australia, the USA and the United Kingdom.
The Australian College of Rural and Remote Medicine is one of two colleges accredited by the Australian Medical Council (AMC) for setting professional medical standards for training, assessment, certification and continuing professional development in the specialty of general practice. It is the only College in Australia dedicated to rural and remote medicine, and is active in supporting junior doctors and medical students considering a career in rural medicine.
ACRRM’s training approach is quite different from most other colleges and based partly around modularised learning. ACRRM Fellows receive full vocational recognition for Medicare General Practice Items and are not just restricted to working rurally, they can practise unsupervised anywhere in Australia.
As a relatively new and small college ACRRM tends to be particularly welcoming to International Medical Graduates.
Number of Fellows: 2013. Post Nominals (FRANZCOG). RANZCOG is the College that deals with the specialty of womens’ and maternal health.
RANZCOG has recently recognised 5 subspecialty fields within its specialty area: Gynaecological oncology, Maternal–fetal medicine, Reproductive endocrinology and infertility Ultrasound, and Urogynaecology.
Number of Fellows: 1275 + 603 jointly with RACP. Post Nominals (FRCPA). The RCPA represents Pathologists and Senior Scientists (working in medicine) in Australasia. Its mission is to train and support pathologists and to improve the use of pathology testing to achieve better healthcare.
It is novel as a college in that it trains non-medical professionals as well.
There is some degree of overlap in training and representation with the RACP. Particularly in relation to the areas of haematology and microbiology. Post fellowship diplomas are also available in anatomical pathology, chemical pathology, clinical pathology, forensic pathology, general pathology, immunopathology and genetic pathology.
A Faculty of Clinical Forensic Medicine also exists within RCPA.
The College of Intensive Care Medicine is the body responsible for intensive care medicine specialist training and education in Australia and New Zealand. The College offers a minimum six year training program, in both general and paediatric intensive care, with a number of assessments, culminating in Fellowship of the College of Intensive Care Medicine (FCICM). The College has over 1000 Fellows throughout the world.
The College of Intensive Care Medicine was established in 2008 and formally took over the responsibility for training and certification of intensive care specialists from the Joint Faculty of Intensive Care Medicine (RACP & ANZCA) on 1st January 2010.
The ACD is the peak medical college accredited by the Australian Medical Council for the training and professional development of medical practitioners in the specialty of dermatology.
The Royal Australian and New Zealand College of Ophthalmologists (RANZCO) is the medical college responsible for the training and professional development of ophthalmologists in Australia and New Zealand.
The Royal Australasian College of Medical Administrators (RACMA) is a specialist medical college that provides education, training, knowledge and advice in medical management. Recognised by the Australian and New Zealand Medical Councils, it delivers programs to medical managers and other medical practitioners who are training for or occupying Specialist Leadership or Administration positions.
Whilst you generally do not require a Fellowship in Medical Administration to work in a leader role, RACMA is the only college based training program where you can become a Fellow in the Speciality of Medical Administration.
RACMA also has significant options for recognition of prior learning.
ACSEP is the professional body representing Sport and Exercise Physicians and Sport and Exercise Medicine in Australasia. Sport and Exercise Physicians are committed to excellence in the practice of medicine as it applies to all aspects of physical activity. Safe and effective sporting performance at all levels is a major focus.
Alongside this is the increasing recognition of the importance of exercise in the prevention and treatment of common and often serious medical conditions, such as arthritis, heart disease, diabetes and many cancers.
The goal of all Sport and Exercise Physicians should be to facilitate all members of the community to enjoy exercise safely to 100 years and beyond, knowing that physical activity provides them the ‘best buy’ to prevent chronic disease.
Number of Fellows: 282. Post Nominals (FRACDS(+/-OMS)).
The RACDS has been existence now for 50 years providing a broad range of activities to enhance the professional development of both general and specialist dentists through individually mediated studies, examinations and continued professional development. It is responsible for the RACDS OMS Training Program.
The OMS Training Program is designed to provide trainees with sufficient theoretical and practical background to meet all current standards available in Oral and Maxillofacial Surgery in Australia and New Zealand.
Eligibility for this program includes the requirement to have both a medical and a dental degree and full registration in both specialties, as well as a year of general surgical experience. So becoming an OMFS surgeon is possibly the longest specialty training program in Australia!
Related Questions.
How To Work Out Which College Is For You If You Are A Specialist International Doctor?
Answer. If you are from overseas it can sometimes be tough to work out how your particular specialty fits into the specialist pathway and the Australian system or in fact how your training may differ from what occurs in Australia.
Here’s an example, in the United States Child and Adolescent Psychiatrists train primarily within the field of child and adolescent psychiatry and probably learn more paediatric medicine than any other form of psychiatry. Whereas in Australia, you have to start out training in general psychiatry and only at the stage of Advanced Training do you undertake significant periods of study in Child and Adolescent Psychiatry.
This can have significant issues for child psychiatrists as much of their training won’t stack up against the program in Australia.
If you are considering working here as a specialist via the specialist pathway, here are a few tips to consider when working out which college fits you:
There may be an obvious first starting point. For example if you field is within the surgical domain, you are likely (but not always) to be covered by the Royal Australasian College of Surgeons. Exceptions might include Ophthalmic Surgeons and Dental Surgeons.
If you have worked generally for many years and are considered a specialist in your country. But you do not have a certificate or have not undergone a formal specialty training program or course. You are unlikely to be granted specialist status in Australia.
If you cannot work out where your particular specialty fits and its not surgically related it probably fits within the Royal Australasian College of Physicians and there many programs Or as an alternative it may be covered by General Practice.
You can actually ask the colleges. They will answer some basic questions before charging you to look at your specialist application. A question likes “this is my subspecialty, do you cover it here?” will be answered free of charge.
Some Things You Ought To Consider If You Are Planning On Medical Interview Coaching This Year. Before You Commit
Are you planning on undertaking medical interview coaching in 2019?
A Wrap Up Of 2020
2020 was another successful year for coaching clients. Demonstrating the value of performance coaching to secure career progression. We managed to help clients secure some fairly competitive posts, including Paediatrics, Cardiothoracics, Radiology and Ophthalmology in some pretty prestigious locations (think Prince of Wales & Royal Melbourne).
Overall I’m probably most proud of helping those trainees who were passionate about their career choice but were being let down by a lack of confidence and poor past advice.
Late last year I did a project for the College of Radiologists looking at their trainee selection processes and how to incorporate things like diversity into the future selection of trainees. I look forward to hearing some results from this work.
Whilst the median number of coaching sessions for 2020 was once again 3. Some coachees, in particular trainees, opted for an additional fourth or fifth session. I clocked well over 500 interview coaching sessions.
Some also approached me for some “last minute” coaching. A once-off medical interview coaching session can be challenging. Particularly in relation to not overloading the coachee with too much new information. However, many doctors reported these sessions as helpful, particularly in being able to calm their nerves prior to the interview and to ask background questions and test out potential work examples to use.
There remains no doubt in my mind, however, that a planned and stepped out coaching approach is far superior and will address higher levels of interview capability and performance.
Key Observations
The format of most interviews remains remarkably conservative. Usually a single small panel of 3 to 5 running for 15 to 30 minutes (shorter for more junior roles, longer for more senior)
The types of questions remain highly predictable and if you practice enough you will likely cover the majority (with slight variation) bar any clinical problem they may put to you
Questions about experience (some what of a waste given they already have your CV), conflict resolution, strengths and weaknesses and preparedness for the position remain popular
Ethical questions, particularly in relation to trainee doctor wellbeing and managing upwards appear to becoming more popular
Most doctors can identify 3 or 4 good examples (good stories) from their CVs that can be used to fit the range of interview questions. Sometimes to more than one question and even if an example is not asked for
Thanks to our community and coaching clients. We have now collected more than 640 interview questions. Providing a useful bank of questions for you to practice upon.
Key Considerations For Interview Coaching
Career coaches often offer medical interview coaching. There are lots of coaches available to choose from if you live in a capital city. Less so in rural and regional places. But video technology now lets you connect virtually and also offers some additional benefits (such as not having to travel and the ability to record sessions easily). Some things you should consider in a coach are the following:
What is the coaches training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process? Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Does the interview coach provide face to face coaching or on the phone or online? Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session? Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching?
To this I would add that your medical interview coach really should know about video coaching in 2020. For obvious reasons.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
My Approach For 2020
I have a passion for medical career development and truly enjoy working with other doctors in a coaching format to reach their goals.
For 2020, I will continue to be offering the 3 session online coaching service as my main format for coaching doctors who wish to improve their medical job interview performance.
As an additional bonus this year I will review your video confernce set up for you. To make sure it looks good for your actual interview.
All this in addition to the ability to offer coaching at a mutually convenient time in the comfort of your own home (or private work area if you prefer). With a recording of each session available to review usually within the hour.
I am always happy to work with doctors on a once-off basis when I can. But I will continue to prioritise coaching clients on a sessional coaching plan.
What Can Be Achieved In a Single Session?
In short. Quite a lot.
We can:
Orientate you to the interview process.
Resolve any queries you may have about the panel.
Practice an opening type question, during which we can also introduce some techniques for relaxing into the interview.
Go over your work examples as they relate to particular common questions.
And review some interview answer frameworks.
What Are The Benefits of a Series of Coaching Sessions?
Everything that is covered in a once-off session can be covered but with more depth and the opportunity for deliberate practice so that improved performance sticks and generalises.
We also use the extended time to develop better examples and practice answering multiple questions in relation to past example and hypothetical frameworks.
Over this time you incorporate relaxation and “panel warming” techniques into your answer approach. You become better at selling your examples and competencies and agile at answering a range of question
Now that Australia appears to have succeeded in dealing successfully with the initial impact of COVID-19 and getting ourselves prepared, there are signs of society returning to some sort of “more normal”. Many doctors, myself included are returning their minds back towards the medical career process. With all the disruptions to the health system and society, in general, it’s not a surprise that there is also a level of uncertainty about what is happening with medical recruitment this year and some uncertainty about how best to prepare. So. We’ve prepared this medical recruitment 2020 reference for you to help you make the right choices.
If you were preparing for a new job in medicine in 2020 then here is a summary of what we advise that you should be doing right now at AdvanceMed:
Keep an eye on the main annual medical recruitment portals. Many have already signalled that recruitment is about to commence.
There are plenty of things you can be doing now to prepare yourself for your next career move in medicine, regardless of whether there is a clear application date, these include preparing your resume, gathering referees and beginning the process of interview preparation.
The majority of interviews this year are likely to be conducted via videoconference, therefore, its important to invest some time and effort preparing to interview on this medium.
Let’s now look at some of these issues in more detail beginning with an assessment of where medical recruitment is up to currently in Australia.
The good news for medical recruitment 2020. Medical Internship is on track.
First the good news. The medical internship recruitment system is going ahead as planned as per the original dates for 2020. All States and Territories will begin to receive applications on 4th May 2020 and close their portals on 4th June 2020. With the majority of intern offers being sent out in July.
This is fantastic news if you are a final year medical student worried about commencing your internship in 2021. But there is one big caveat. You do have to still graduate first. And it’s reasonable to say that the majority of medical school programs have been put into disarray in Australia due to concerns about exposing medical students to COVID-19, diverting normal supervisory resources to COVID preparedness and enforcing social distancing in clinical environments, which has significantly challenged clinical placements which are absolutely important in the final years of medical school.
The Australian Medical Council, Medical Board of Australia and Medical Deans have been working together to put in place changes and processes to assist medical students in completing their education on time, which should help.
But one of the paradoxical outcomes of Australia being more successful in dealing with COVID-19 is that there hasn’t been a mad rush to adopt alternative models of placing medical students in pre intern posts as has occurred in other countries like the United Kingdom and the United States.
So it remains somewhat uncertain whether there may be a decline in the number of intern positions taken up in Australia in 2021.
The Not So Good News. Some Colleges have delayed Selection into Training.
The not so good news is that some colleges have made announcements in relation to delaying their normal selection into training processes. In particular, the Royal Australasian College of Surgeons has indicated that its selection into the various SET programs for 2021 is delayed until further notice. My information is that RACS is hoping that they may still be able to conduct their normal panel interviews in person later in the year.
Other colleges have indicated that there may be some disruptions but that selection into training will still occur. Many like the Royal Australian and New Zealand College of Obstetricians and Gynaecologists have indicated that interviews will be conducted using videoconferencing.
Of course, some colleges have more “skin in the game” for selection into training posts than others. So there has been little or no impact for example on the Royal Australasian College of Physicians, which generally selects trainees for Adult Medicine and Paediatrics into basic training after they have secured an employer post. And does not conduct interviews for selection.
The Mixed News. There Is Some Disruption to the Annual RMO Campaigns.
The mixed news is that the impact of COVID-19 preparedness and uncertainty around some college selection processes has caused some of the State and Territory Departments of Health to place notices on their jobs board indicating that there will be some impact on annual medical recruitment related to COVID-19.
In particular, NSW Health has, as of the writing of this article, placed a pause on its process and indicating it is considering a range of options for medical recruitment. And the Postgraduate Medical Council of Victoria has placed a pause on its selection to Radiology training posts.
However, a scan of most of the other State and Territory medical recruitment campaign sites, for example, Western Australia and Queensland, appears to indicate that these jurisdictions are on schedule to open as planned.
So What Does This All Mean?
My interpretation of all this information is that there is likely to be a small level of disruption to the annual medical recruitment processes across Australia. However, the combined fact that internship is on track and that many of the States and Territory RMO campaigns appear to be “situation somewhat normal” would indicate that annual medical recruitment is likely to commence on or near to normal schedule across Australia. States like NSW and Victoria are unlikely to totally abandon or significantly delay their systems if other jurisdictions are going ahead.
Expect, perhaps, that some positions, in particular ones linked to college selection, might be delayed to a later round and recruited to a little bit later than usual.
How Best To Prepare Yourself In These Uncertain Times.
So what advice do I have for medical trainees who would like to know how they can prepare themselves for medical recruitment in 2020.
Enact Your Medical Selection Plan Now.
My first piece of advice would be to try and treat the process as you would normally do. That would mean for most doctors that you should be enacting the first part of your plan now if you have not already done so.
Of critical importance will be your Resume. There’s plenty of advice on this blog about how you can make this document stand out. You should be aligning this with the competencies being sought for the position/s you are intending to apply for. Think about adding in a story about COVID-19 2020 that shows off one of these competencies. Ensuring that you have relevant, recent and diverse referees to speak on your behalf is also something you can be doing now.
You should also be thinking about starting your interview preparation. Many candidates that I coach start this process far too late. In my experience, there is little risk of starting too early (you can always pause for a bit if you lose momentum). Interview skills are like muscles. They need regular training to help you show your best on the day. The problem is. If you haven’t interviewed for a while. This muscle is likely to have atrophied.
Review Your Video Conference Set-Up
Finally, it’s important to understand that your next doctor job interview is most likely to be conducted on something like Zoom. There are significant differences in interviewing on video versus in person. Both from a technical perspective as well as from a practice perspective.
You should definitely be reviewing and modifying your videoconference set up and your environment as well as actually practising interview questions using video. The latter is actually a good idea in general as it affords you the chance to record and review your performance.