Come back regularly as we endeavour to give you the most comprehensive information on the doctor job application process. All things medical job-related.
If you are thinking of working in Medicine in Australia you may naturally want to know exactly how much you will earn. Having worked in the Medical HR field for over two decades I thought I would challenge myself to write you a comprehensive post to cover as many possibilities as could be thought of.
But first let’s get the question of the range of doctor salaries dealt with. As of March 2019, A doctor salary will range from a low of $68,000AUD per annum as an Intern in the State of NSW to a possible high rate of $393,467AUD on average per annum for a Surgeon (according to Nine Finance).
Now let’s dive deeper. Because most doctors, can often earn a lot more than average, particularly by working additional hours and working in the private sector. Let’s also look at what various types of training doctors make in pay before looking at the various specialties and some other categories of doctors.
Trainee Doctors.
Specialists.
This is where it starts to get a bit more difficult
Career Doctors.
Additional Benefits.
Related Questions:
Question. What Costs Are Involved in Becoming a Doctor in Australia?
Answer.
Question: Do All Doctors Get Superannuation?
Answer.
Question: Do Doctors in Australia Get Health Insurance?
Resident Medical Officer. Or just plain “Resident”. Is the job title that is most commonly applied to Australian doctors working in their 2nd year of Medicine in Australia. This title can also be given to a doctor working in their 3rd year or later. However, Resident is not the only title used and the situation can be confusing. Add to this, that being a resident doctor in Australia is not the same as being a resident doctor in a country like the United States. What trainee doctors get called and what doctors salary they get paid after their internship can become terribly confusing. Both for Australian doctors as well as doctors from other countries. So I pulled together this post to help clear it up.
Firstly, let’s address the key question. What does a Resident Doctor get paid in Australia? As of 2019, a Resident Medical Offcier (RMO) in Australia will make anywhere between $72,837, in Tasmania, which is the lowest rate and $86,328 AUD in Western Australia, which is the highest rate. Bear in mind that this is base annual Full-Time salary. Most Resident doctors are employed Full-Time but work additional overtime hours as well as shiftwork. So take home salaries can increase rapidly and it would not be unreasonable to see about 25-50% more salary on top of this.
To further clarify, these are the rates paid to doctors in their second year of work in the hospital system. Or what is commonly referred to as a Postgraduate Year 2 (PGY2) doctor. The rates do increase if you are more experienced.
So let’s dive in a bit deeper to the situation. To see how pays compare across the various States and Territories in Australia. As well as what sort of title you might have if you are working at a PGY2 level in one of those particular States and Territories.
Resident Doctors Salary By State and Territory
State or Territory
Common Title
Base Full Time Annual Pay (AUD)
Western Australia
Resident Medical Officer
$86,328
Northern Territory
Resident Medical Officer
$82,731
South Australia
Resident Medical Officer
$80,041
Australian Capital Territory
Resident Medical Officer
$79,682
New South Wales
Resident Medical Officer
$79,648
Queensland
Junior House Officer* OR Resident Medical Officer
$79,413
Victoria
Hospital Medical Officer*
$79,391
Tasmania
Resident
$72,837
Information accurate as of February 2019. Rates of pay are regularly altered on an annual basis at different times depending on the State or Territory industrial framework.
*Interns (PGY1 doctors) are also employed as Junior House Officers and Hospital Medical Officers in Queensland and Victoria respectively. So the titles are interchangeable and you should check if the position is for a PGY1 or greater.
An Explanation of Titles
As I have noted the most common position title you will probably see in most States and Territories is some version of “Resident Medical Officer”. So you might also see just plain “Resident” or the abbreviated version of “RMO”.
If you see “Senior Resident Medical Officer” this means the position suits someone slightly more senior. Usually someone in their PGY3 or third year of medicine.
However, employers generally have a choice or even free reign to call these positions whatever they like. Some will stick to the title under the Award or Enterprise Agreement (see below). Some will go for the more generally understood Resident Medical Officer.
But you may also see titles like “Medical Practitioner” or “Trainee” or “Unaccredited Trainee.”
Addressing the Confusion.
If you are confused as to what level the position is there are a few things that you can do:
Firstly, you can look at the details of the job description:
It will often tell you the level under the Award or EBA.
There may be a description of how many years of experience you need.
You might be able to infer that it is a resident level job because you will report to Registrars or specialty trainees. If you are reporting directly to Consultants then it is a much more senior position.
Finally, you might be able to work it out from the salary range.
If none of that works you can try contacting the person who advertised the position. They will normally have an email contact and often a phone number listed.
Western Australia Leads Again.
There are some interesting observations about this list when one compares it to the Intern pay table. Firstly, Western Australia remains the clear leader in trainee doctor pay rates. And in fact, Western Australia continues to stay ahead as one enters into the specialty trainee doctor pay scales. On at least an annual base salary basis it has to be said that Western Australia pays its trainee doctors the best.
The strong improver on the list is NSW. Which leaps over Tasmania and just squeezes past Victoria and Queensland to no longer be last. Tasmania is in fact well and truly last being almost $7,000 in the rear of Victoria which is second last.
The two largest States in Australia (by population), being Queensland, Victoria and NSW are actually extremely close in what they pay Resident doctors. There is really not that much difference between them.
Not All Are Equal.
But this is oversimplifying the situation.
Whilst Victoria and NSW pay their Resident doctors approximately the same rate of pay. The Enterprise Agreement for doctors in Victoria (see below for what one of these is) is arguably the most modern in the country. And includes a suite of additional benefits which are not given to doctors in NSW. NSW arguably has the most out of date Award of all the trainee doctors Awards or EBAs in the country.
There are some things you get when you work as a Resident in Victoria. Which you don’t get when you work as a Resident in NSW. These include a provision of up to $3,000 for continuing professional development, as well as specific provision examination leave as well as conference leave.
How Are Doctor Pay Rates Determined in Australia?
You may be wondering why there is such a difference in pay rates for trainee doctors in Australia? And also why I am quoting you pay rates by State and Territory with confidence? And not digging into individual rates of pays at certain hospitals or health networks.
To understand all of this one has to briefly explain what is called the industrial relations system in Australia. Before Australia became a sovereign country it was actually already a collection of individual States. With their own parliamentary and judicial systems based on the UK system. These systems continued with the Federation of Australia, with a division of authorities and responsibilities between the Commonwealth and State parliaments. One responsibility that was maintained by the State’s was the ability to determine labour laws. Or the laws that regulate who can work, how and when and for how much.
On top of this federal system, Australia has always had a strong trade union movement that has worked collectively for its members to secure improvements to work conditions. Over time a system developed in Australia to determine disputes between workers (represented by trade unions) and employers on both a State and later Federal level.
The Arbitration System.
This system was and is called “arbitration” and basically involves a court hearing both sides arguments and making a determination.
So basically whenever there is a dispute over conditions it is determined on an industry basis and either for the whole State or the whole country. Disputes are generally not heard on an employer or workplace basis. Although this has changed a bit of recent times.
The arbitration courts developed and updated legal documents called Awards. These Awards contained all the rules about what certain workers were required to do, how they got paid and what other “entitlements” (such as leave) they would have.
Awards are determined based on industrial classifications. So for example, in NSW there is an Award which is called the Public Medical Hospital Officers Award which covers all trainee doctors employed in NSW hospitals.
More recently in certain States the Award system has altered slightly to a process of what is called enterprise bargaining. Essentially, the employer and the union representing the workers agree to put aside the Award and develop a contract that both parties agree to.
Awards and EBAs Outline the Conditions of Employment for Everyone.
Whether it is an Award or Enterprise Bargaining Agreement (EBAs) both documents outline the conditions of employment for all employees of that classification.
Awards and EBAs normally outline rates of pay based upon years of experience with some progression steps. So for example in Tasmania, you will start out as a Medical Practitioner Level 1 (Intern). And after one year automatically progress to a Medical Practitioner Level 2 (Resident year 1). And the next year move up to a Medical Practitioner Level 3 (Resident year 2). But you have to be appointed to a Medical Practitioner Level 5 (as either a Senior Resident year 1 or Registrar year 1) before you can progress up to this particular salary point.
So there are names attached to the classification or grading levels under the Awards and EBAs. And these are often also used for the actual position title when you see a job advertised.
Additional Benefits.
As I have mentioned most trainee doctors work full time and on top of this are expected to do a certain amount of overtime. As well as what are called penalty rates on top of their normal work hours. Normal work hours in Australia are generally Monday to Friday 8.30am to 5.00pm but can also sometimes vary to be something like 7.30am to 4.00pm.
You generally work 40 hours per week if your are full time. So if you work 8.30am to 5.00pm you get paid 8 hours for that day’s work. The additional 30 minutes is meant to be an unpaid lunch break.
Penalty Rates.
Penalty rates are extra amounts of pay you accumulate per hour for working your normal hours in a less favourable time period. So, for example, working evening shifts or night shifts or working on the weekends. You might get paid anywhere between an additional 25% to 75% for a penalty rate shift depending on how undesirable it might be.
Overtime.
Overtime is different from penalty rates in that whilst you are also working outside the normal working hours you are doing so on top of your normal 40 hours per week. Overtime rates usually start at time-and-a-half, i.e. you get paid 150% of your normal hourly rate and in most circumstances quickly escalate to double-time (200%).
The system for penalty rates and overtime does vary a little bit amongst the different State and Territories a little bit. So you need to check out the individual Awards and EBAs to know exactly what you get paid and for what.
Some Other Benefits.
There are a range of other benefits that you get when working as an employed doctor in Australia.
On top of your salary, your employer is required to pay an additional 9.5% into a superannuation fund to assist with your retirement.
As an employee, you are covered by workers compensation for any injury or accident that might occur at work. Although payouts are often fairly poor and below what most professionals earn. So you may wish to consider taking out additional income protection insurance.
If you are asked to be on-call you will get a small allowance for this and be paid if you are called back into work.
You may get an allowance or even a mobile phone provided to you if you are required to be on call.
You might get some meal allowances for shifts.
If you have been seconded a reasonable distance from your normal place of appointment you will generally be provided with free temporary accommodation (you may need to pay a bond) and a travel allowance, for example, a free air ticket back home every 13 weeks or so.
You will get at least 4 weeks of annual leave per year.
Most doctors will also get one extra day off per month. Called a Rostered Day Off or RDO.
You will get a certain amount of sick leave every year which you can accumulate if you don’t use.
You also get access to other types of leave, such as leave to take your child to the doctor.
What About Health Insurance?
Unlike in the United States and some other countries Australian employers do not provide health insurance. If you are a citizen or permanent resident you will be well covered for basic care under the Federal Government’s universal health care scheme. If you are on a temporary visa you will likely need to take out some form of insurance. Unless your country has a reciprocal agreement in place (for e.g. between the United Kingdom and Australia).
Related Questions.
Question: What About Medical Indemnity?
Answer.
Medical Indemnity or professional liability insurance is not a requirement if you are only working as a doctor in a public facility or health service. This is because you are indemnified by the employer’s insurance. However, it is generally advisable to sign up to one of the Medical Defence Organisations anyway as it generally only costs a few hundred dollars and means that you have an independent provider to turn to whenever you have a medico-legal concern or question.
If you are working in general practice or a private hospital then you will need some form of indemnity. Again, this may be provided for you. But you should check the details of the cover and particularly ensure that “tail cover” is in place (cover for after you leave the position).
Question: When Do You Become a Registrar?
Answer.
Generally speaking in Australia most doctors enter into vocational or specialty training at postgraduate year 3. These positions are most commonly referred to as “Registrar” posts. But again there are other titles and it can become just as confusing. I plan to write a post about this matter at a later date.
In some cases you can enter specialty training as soon as PGY2 and of course you can also delay it to later into your training.
If you see a position advertised as “Registrar” or “Trainee” it is generally a specialty training post. If you see the words “Unaccredited Trainee” this means that you will work at the level of a specialty trainee but won’t receive any formal training. Unaccredited trainee positions can be exploited by hospitals as they are not subjected to College accreditation and standards.
Question: How Much Does An Intern Get Paid?
Answer.
Generally somewhere between $68,000 and $79,000 AUD as a base salary. For more information go here.
Question: Can I Negotiate My Pay & Conditions?
Answer.
Unlike some other countries, individual pay negotiation is unusual in Australia
This is not to say that you cannot ask about certain things. But you have to bear in mind that the system is designed to be equal for everyone else at your same level, so employers will be reluctant to give you something that might give you an advantage over colleagues.
Employers will also generally be limited to changing things according to how they are already covered in the Award or Enterprise Agreement (see above) or things that are not specifically covered by the Award or Enterprise Agreement.
So examples of things you might be able to negotiate are:
Your commencement grade. Some employers will try to offer to employ you at the lowest grade possible, ignoring your past experience. You should always check on this as once you accept a certain pay grade its hard to negotiate to change it. Whilst you are in the “acceptance phase”, i.e. you have the contract you may be able to highlight to the employer that you have in fact worked more years as a doctor already and should be started as for example a Resident Year 4, rather than a Resident Year 2.
Where you are going to work. Often as a Resident you will be employed to a primary hospital which has secondments or even just a network of locations. You should always ask questions about the types of rotations and see if you can lock in where you will be working for the length of your contract. This may be particularly important if you need certain rotations to satisfy the Medical Board of Australia for registration purposes or you have specific personal or family arrangements. You probably won’t be able to get out of a secondment but you might be able to choose where you go and when you go there.
Relocation expenses. Employers generally have some discretion to pay for relocation because this issue is generally not covered by the Award or EBA and its a once-off expense. It may depend on how desperate they are to have you. But it doesn’t hurt to ask politely.
If you have a question about Resident job titles or pay conditions. Feel free to post it below.
Doctors like all other professionals experience career challenges. Sometimes these challenges are about moving upwards in your career. Sometimes they are just about dealing with tricky challenges in your current role. Whatever the situation a career coach can often be a useful resource to help you out.
So if you are working as a doctor in Canberra, what are your options for career coaching? Well, like most large cities there is a range of career coaching options in Canberra. Some of the more popular services in Canberra, include Katrina Howard and Kim Vella.
However, our search was unable to find a career coach specializing in medical practitioners or doctors. So you may also wish to consider working with a coach remotely using video-coaching.
Let’s talk about some of the ways that doctors might use a coach for their careers.
Interview Coaching.
Interview coaching is an obvious place for a doctor to start with coaching. Interview coaching is a way for some doctors to improve upon their interview skills prior to a formal job interview. Given the high stakes of some medical job interviews its normal to be worried about giving your best performance or that nerves might get the best of you on the day.
During interview coaching, a doctor meets with a professional coach to learn strategies for being more relaxed about the interview process and of course to perform better.
So should you work with an interview coach? And if so, how can you find one that suits your needs?
The most obvious reason is that interview coaching can help increase your chances of getting a job. There are a number of ways this can occur.
Coaching can help you overcome any nerves or anxiety you have about the process.
Coaching gives you a chance to experience answering many different interview questions.
Coaches provide you with feedback to help improve your responses during interviews.
The more you practice with a coach, the more confident you will become. By engaging with a coach you are also ensuring that you commit to your own practice regimen, which is important for a good performance.
Some reasons you may want to consider engaging a doctor interview coach:
It’s been awhile. If it’s been a few years since the last time you interviewed for a doctor job or if your last interview was fairly simple and you anticipate this one will not be the same, then a coach can help you rehearse and regain your interview confidence.
You get nervous before interviews. A little bit of anxiety is good going into an interview. But too much anxiety can affect performance. Practicing with a coach can help you feel more comfortable, relaxed and prepared.
You get interviews, but not offers. Often its difficult to get honest feedback from medical interviews. A coach may be able to help work out what is going wrong for you.
You are not sure about something on your CV. Maybe you have had to have a break in work. Or your last job didn’t go so well. Are you perhaps switching specialties. A coach can help you with how to tell the right story in relation to these sorts of issues.
Its your dream job and you want to land it. A coach can help with feeling confident in these situations.
On the other hand, if you’re a confident interviewer and have always tended to perform well during interviews, then a coach may not be necessary. But you might still want to think about practising a few times with a friend or a colleague.
Types of Interview Coaching
There are many types of interview coaching. Some coaches meet with you in person, and others speak with you online or on the phone.
In general interview coaches work on something called “performance coaching”. Think of it like a sports coach working with an elite athlete. A key element is practice with feedback. The more practice and the more immediate the feedback the better.
If you meet the coach in person or online, they can also help you develop effective visual communication. The coach can work with you on facial and body expressions that convey trust and show active listening.
Coaches may also help you with other elements of the interview, including how to ask the right questions of the employer, how to research the job and the panel and even some advice on how to dress.
How to Find a Doctor Interview Coach
There are lots of coaches available to choose from in a capital city like Canberra. Career coaches often offer interview coaching. Some things you should consider in a coach are the following:
What is their training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process. Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Do they provide face to face coaching or on the phone or online. Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session. Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
Other Types of Doctor Coaching
Some of the other reasons that doctors may seek the aid of a career coach include managing issues in their current role as well as longer term career planning. Here’s a couple of common examples:
Entering into Management Roles
At some point in time most doctors get asked to take on some form of formal leadership position. This can be quite a challenging time as often this role transition seems like it has come with little warning or time to prepare. One of the great failures of our medical culture is to inadequately prepare doctors for leadership roles.
So the newly appointed Head of Department or Acting Clinical Director can suddenly find themselves in what seems to be a very foreign land of budgets, people management, risk registers, strategic plans and the like.
More often than not. Doctors can make this adjustment. A career coach can encourage doctors in leadership roles to take a positive and learning attitude to the new role and reframe challenges to see novel solutions. They can also often make suggestions around training or skills development which might assist.
One process that is often suggested in these circumstances is a 360 Feedback, which helps the new doctor manager get some feedback from their team as to how they are performing and what developmental areas they may wish to look at.
Thinking About Leaving Medicine
Burn out is a significant problem in our profession. Many doctors can feel like they have ended up in a career in Medicine which is no longer satisfying them. But they also struggle to see what other options they may have. If they talk about leaving medicine with their colleagues or even friends and family they are often met with well-meaning but largely unhelpful suggestions about how they might be able to keep going or even comments like “but it would be such a waste if you left medicine”.
The role of the career coach in such circumstances is to take a neutral view on the end outcome. Perhaps the doctor hasn’t seen all the possibilities quite yet? Perhaps leaving medicine is one possibility, but what exactly does this look like?
Seeing a career coach at such existential times in a doctors career can really help to see the problem in new ways and move through a fog of indecision.
If you would like to discuss more about coaching for doctors, leave a comment below.
If you would like to check out the types of doctor coaching services that I provide click on the link below.
For many international medical graduates (IMGs) the pathway to being registered as a doctor involves the Australian Medical Council exams. But for doctors who have worked in more than one country already there are sometimes other options, such as the PLAB. But you need to be careful that you meet all the required criteria for your PLAB to be recognised.
Doctors sometimes ask whether the Professional Linguistics Assessment Board (PLAB) is accepted or recognized in Australia. The simple answer to this question is yes. The PLAB will be recognized by the Medical Board of Australia and this will mean that you are not required to sit the AMC exams. You will be able to apply for registration via the competent authority pathway. As a bonus, you will also be exempt having to prove your English language proficiency. However, it is important to check the full requirements. In particular, doctors who complete the PLAB must also complete 12 months of supervised training in the United Kingdom. If you have not completed this training your PLAB will not be accepted.
Lets dive a little deeper into the requirements of the PLAB. Why it is that the PLAB is accepted in Australia. As well as the other options for not having to undertake the AMC examinations.
What is the Purpose of the AMC Examination?
The AMC Examinations are the main route by which doctors from most other countries can apply to become registered as a doctor in Australia. Without medical registration in Australia it is illegal to work as a doctor.
The AMC exams consist of a written (multiple choice) examination and clinical examination and are set at the equivalent standard as what would be expected of an Australian medical school graduate commencing their first working year in Australia, which is called an internship.
Australia sets high standards for medical practice and therefore, with a few exceptions, we do not directly recognize the output of medical schools from many countries. So the AMC Examinations have been established as a process for testing the capability of IMGs.
So Who Needs to Sit AMC Examinations?
If you have graduated from the United Kingdom, New Zealand, Republic of Ireland, Canada or the United States you are not able to sit the AMC exams. Because you are not required to do so.
If you are from any other country you are able to sit the AMC examinations. However, if you have specialist qualifications you probably want to try the specialist pathway instead.
Also, if you are not from the United Kingdom, New Zealand, Republic of Ireland, Canada or the United States. But have worked in the United Kingdom, New Zealand, Canada or the United States. You may also be able to avoid the AMC Exam process and can apply via Competent Authority.
Notice though we did not say “Republic of Ireland”. If you are an IMG who has worked in the Republic of Ireland before this does not help you avoid the AMC exams.
Read on.
The Competent Authority Pathway.
The Medical Board of Australia recognizes the medical school training systems of the United Kingdom, New Zealand, Republic of Ireland, United States of America and Canada as equivalent to the Australian medical system and therefore does not require medical graduates from these countries to sit additional examinations to prove that they are capable of working as a doctor in Australia.
New Zealand medical school graduates are treated as identical to Australian graduates. In fact New Zealand Medical Schools are accredited by the Australian Medical Council as well. New Zealand doctors can apply directly for general registration, so long as they have completed an intern year in either Australia or New Zealand.
Graduates of the UK, Rep Ireland, US and Canada can apply for registration in Australia so long as they have also completed the basic requirements for being registered as a doctor in their country. You will also need a job offer prior to applying for registration. So long as the Medical Board is satisfied that you will be provided with sufficient level of supervision for 12 months you can work under “provisional registration”. Once this period is complete and you have returned satisfactory supervisor reports you will be able to apply for general registration.
If You Are Not From the UK, US, Ireland, New Zelaand or Canada You Can Still Come Under the Competent Authority Pathway.
Some doctors work in a range of countries. Countries like the UK and Canada have similar systems to Australia for allowing IMGs to work in Australia.
So if you have completed any of the following:
PLAB in the UK;
NZREX in New Zealand;
USMLE in US; or
LMCC in Canada
You are also able to apply for registration via the competent authority pathway and can skip the AMC exams.
However, as mentioned earlier. You do need to do all the steps. One thing that can sometimes catch IMG doctors out is that they have completed all the examination steps of one of these processes BUT NOT completed the supervision steps. So, for example, have not completed a Foundation Year in the UK. Or have not completed 2 years of ACGME accredited training in the United States.
The Specialist Pathway.
The Specialist Pathway is for doctors from any country. Competent Authority or Standard Pathway. It enables a doctor to apply to be recognised as a specialist in Australia.
So its another pathway which avoids the AMC exams. Which in the case of many specialists may be quite daunting as it will have been some time since you have studied such a broad range of medicine.
Rather than going through the AMC examination process. The specialist pathway places you directly in contact with the specialist colleges. Who do a review of your training, qualifications, and experience to determine whether you are comparable or not. If you are found to be comparable. You will be offered a period of registration to demonstrate your performance and you may also have to sit further specialty examinations.
Once again, you need a job offer to complete this process.
If you are not found to be comparable you will have to either sit the AMC examinations or apply for competent authority if that option is available to you.
I Really Don’t Want To Do The AMC Exams. Are There Any Other Options?
There is one final option but its not particularly popular as it is time limited, has certain restrictions and is not meant as a mechanism for making a permanent move to Australia.
This option is called the Short Term Training in a Medical Specialty Pathway. It is an option for gaining either provisional or limited registration for a period of up to 24-months to undertake additional specialty training in Australia. This registration category is generally made available to Advanced Trainees or Junior Consultants from other countries who are looking to augment their training experience.
And. Once again. You do need a job offer to apply for the registration.
Barring enrolling in medical school in Australia. There are no other options for not doing the AMC exams.
Related Questions.
Question: Do I Need to Do The Foundation Program to Complete the PLAB Requirements for Australia?
Answer.
It is generally a good idea if you can successfully complete the 1st Year of the Foundation Program in the UK. Note you only need to complete one year.
However, if you are unable to do this the Medical Board of Australia will accept alternative evidence that you have worked successfully in similar posts:
This is the direct quote from the Medical Board documents:
There are two ways in which you can demonstrate that you meet the ‘12 months supervised training (internship equivalent) in the UK’ component of the eligibility criteria for category A (as per guidance initially provided in August 2015):
1. Provide evidence of ‘12 months supervised practice/training in an Approved Practice Setting in the UK’. Acceptable evidence would include: a. confirmation in writing from the hospital(s) and/or employer(s) that you have satisfactorily completed 12 months supervised practice/training in the UK, and b. confirmation in writing from the hospital(s) and/or employer(s) that the practice setting is an ‘Approved Practice Setting’.
OR
2. Provide evidence of ‘a minimum of 12 months practice in the UK’2 . Acceptable evidence would include: a. confirmation in writing and/or certificate of service from the hospital(s) and/or employer(s)that you have had a minimum of 12 months practice in the UK.
You will also need to provide evidence that you have ‘successfully completed the Professional and Linguistic Assessments Board (PLAB) test since 1975’.
Answer. This is a complex question. Its probably best to assume that you do. Even if you are coming from an English speaking country. Until you have established that you do not.
Generally speaking if you can prove that you have been high-schooled in English and studied Medicine in English you will be fine.
However, there are many circumstances where this has proven to not be the case. Even choosing to work for a small period in another country where English is not the first language can result in you having to sit an English test.
For doctors who have completed the PLAB and NZREX. The Medical Board will generally exempt you from the need for an English Test. This is because the PLAB and NZREX include an examination of English.
Question: Can I Count Part of My PLAB or USMLEs Towards the AMC Multiple Choice Examination?
Answer. No. The AMC will not recognize partial completion of any of these examinations as a proxy for the exam here.
For most medical students the point at which you need to think about compiling a Curriculum Vitae (CV) or Resume comes in your final year of medical school. This is the time when you need to think about applying for a job for after graduation. As a doctor who has seen 10,000+ CVs in his career I’ve put together some tips for the medical student CV, including how it may differ from other types of doctor CVs or medical resumes.
But before we dive into these tips. Let’s look at what the key aspects of a medical student CV are. In order to compile a good quality medical student CV, you should ensure the following vital elements are covered:
The most prominent element on your medical CV should be your name. This is what you want potential employers to remember.
You should have clear and professional contact details. So they can get in touch easily.
A personal statement is highly recommended. As you then get the chance to control the narrative (not the employer).
Your education history will take prominence over work history, which is different from the way it goes for the rest of your career. You should, therefore, try to continue “the narrative” in this section and signal some of your special achievements during this time.
There are of course other things which should go on your medical CV. But the above are in my experience the most critical elements and if you focus upon these then you will have a very good first page for your medical CV and this is the bit of your CV that actually gets read.
9 Tips For Compiling A Good Quality Medical Student CV.
Tip 1. Don’t Leave It Till Your Final Year of Medical School.
It seems obvious to say this but you should really be thinking of making a CV the moment you enter medical school. Keep an original copy somewhere that you use to keep a record of your achievements over time. You can then use this to make shorter variations when it comes time for applying for jobs.
The term CV is actually a misnomer. A CV technically is a full record of all your career information. For doctors who have worked a while this document can get quite big. With the various jobs they have done, the courses, conferences, papers published etc…
The document you are normally putting forward is generally more akin to a resume which is a tailored synthesis of your career put against the actual role you are applying for.
At the very least start thinking about your medical CV in your penultimate year of medical school. This is because you want to giver yourself the time to collect the number of referees you may require on the document. Normally this is a minimum of two.
Tip 2. Leave the Photo Off (Unless Specifically Requested). Make Your Name “the Hero”.
Occasionally you may be requested to include a photo as a formal requirement. If so do then. Otherwise leave it off and use the space to make your name the biggest item on the front page. You want the reviewer to remember you name as they hopefully put your medical CV into the “for interview” pile.
Tip 3. Include a Personal Statement.
Personal Statements or Career Goal Statements are really important. Once, you realize how long it takes (or doesn’t take) to review your CV. You will realize the importance of a summary statement at the top of the CV that lets you tell the story of your career and doesn’t leave it up to the reviewer to make up.
For a medical student CV I tend to recommend a Personal Statement over a Career Goal Statement. It can be seen as just a little too presumptuous at this stage to be declaring your specialty intentions at this point.
Concentrate on talking a little bit about:
Why you choose a career in Medicine
What your interests are. You can broadly allude to your career intentions, for example use terms like “critical care”, “interested in procedures”, “rural medicine”. Make sure though that you back this up with some evidence from your medical school about how you pursued these interests. So it doesn’t come off as a second thought.
And then finally try to throw in some value for the employer. What skills do you bring that add some thing additional that others perhaps do not. Again, this could be some of the extra stuff you did throughout medical school or for many it might be skills you developed in a career prior to medicine.
Tip 4. Continue The Use of Narrative and Sell Your Educational Achievements.
Because you don’t have a medical work history its very important that you signal any special achievements you had during medical school. You don’t have to just talk about your formal education in this section. You can bring in other things you may have done during this time. A classic is tutoring other students or other forms of part-time work.
Most students have to work on one or two projects or some form of research during medical school so you could also talk about the outcomes of this work.
If you were on a committee talk about what that committee achieved during the year.
If possible try to quantify your outcomes. If, for example, you helped organise a rural medicine one-day workshop state how many attended.
Don’t just put down that you were the Secretary of the Medical Society without talking about your achievements. Employers are acutely aware how much a waste of time most committees are. So they will assume that you took up the position to add to your CV and did nothing during that year.
Tip 5. Your Work History Prior to and During Medicine is Of Interest.
Your work history or “work achievements” prior to medicine is of interest to employers. It may help to make you a more unique candidate. Definitely put this down its not a disadvantage.
I once had a medical student ask me if they should put down the fact that they were an Executive Assistant in a prior career. My answer was absolutely! Interns are in fact glorified Executive Assistants for a fair bit of the time. And EAs are well known for their ability to get work done, time manage, juggle tasks and be the linchpin of teams.
Tip 6. Stick to a Simple Style and Format.
Try to avoid too much formatting to your CV until you are close to completing it. Ideally, choose one font-type and don’t vary the size too much. A contrast in colour is ok. As is the use of a colour block with whit text to highlight important things like your name.
Avoid going too crazy with underlined words and bolding and italics. Also try to stick with only one level of indenting and bullet points. Otherwise it can start to look a bit chaotic.
Also, check that sections are not being split between pages. If they are pad things out a bit so that new sections start at the top of the page.
Tip 7. Start a LinkedIn Profile.
Now that you have completed all that work in compiling your CV. Why not go the extra step and set up a LinkedIn profile if you have not already OR update it if you have.
There are a number of reasons for doing this but the prime one is that employers now do Google searches on prospective employees and LinkedIn profiles rank well on Google so it once again gives you a chance to control what is being said about you, as well as manage your online reputation.
In this case make sure that you do include a photo as it is expected on LinkedIn.
Tip 8. Your CV Should Be As Long As It Needs To Be And No Longer.
I see so much rubbish on the internet about how a Resume should be no longer than 2 pages or in some instances 1 page. The logic being that if you can’t synthesise your career down to that length to make a winning proposition to an employer. Then you are no go.
I’m calling BS on that.
Sure I have seen some really good tight doctor CVs or Resumes that have managed to get down to 2 pages. But these have generally either been medical students or interns.
I have also seen people try to cram all their information on to 2 pages and make it look a mess because the font-type size is too small.
Once you have worked as a doctor for a while you accumulate a lot of work experience and other good stuff. So generally this takes a few more pages to fill out. Normally this is 4 pages but if it requires more then fine.
Remember employers mainly only focus on the first page in any case. Concentrate on getting this right and then include other things that you think support that first page.
Tip 9. Don’t Get Overly Concerned About How Much a CV Matters At This Point.
Perhaps I should have put this point first. But I wanted you to understand all the other points above first. In most cases you do need a CV. So you might as well make a good one.
That being said. Because there is no medical work history to put on your CV. Employers will not pay as much weight to it. Employers know that the best test of whether someone is good for the job is to try them out in it. And the second best is if they can relate similar succesful job experiences from the past.
So don’t get too concerned if you feel that yours doesn’t have much of interest on it.
Recommended Format For a Medical Student CV.
The format I recommend for most Medical Student CVs is as follows:
Big Bold Name at the very top.
Contact details just underneath or to the right hand side. You really just need a mobile phone number and a professional looking email address so they can contact you. If you have social media profiles such as LinkedIn you can include these as well.
Short Qualification Summary just below as well as any other pertinent information such as citizenship or visa status.
Personal Statement. See Above.
Education Achievements. Note we use “Achievement” rather than “History”
Work Achievements
Other Headings
Referees. Always Come Last.
By the time you have finished the Education Achievements Section you are probably going to be onto the second page. After Work History you can pretty much use what ever other headings you choose in the order that you feel represents you best. But remember you can always bundle some of the good stuff up under your Medical School description as well.
So some other headings you may wish to use include:
Research
Publications
Academic Achievements
Courses
Professional Development
Teaching
Writing
Skills
Volunteer Work
Languages
Quality Improvement
Leadership
Awards
Certificates
Committee Work
Below is an example:
Related Questions.
Question: Are There Cases Where I Do Not Need a CV?
Answer: For most Intern applications in Australia you need to supply a CV. For NSW you do not need to supply a CV unless you are applying via the Rural Preferential Pathway.
Question: How Do I Put Together a Medical CV As a Trainee Doctor Or Consultant?
Question: What Sort of Referees Should I List on My CV?
Answer: As a general rule you should have at least one referee who has worked with you in a supervisory capacity in the last 12 months. You don’t necessarily have to have all doctor referees on your CV. But you should have at least one. Try also to have a diverse range of referees on your CV. For a more comprehensive overview of referee selection and how to list them check out the related post.
Question: What Is The Best Way To Proof Read My CV?
Answer: Proof reading of CVs is important. Even small typographical errors can be seen as an indication of a lack of eye for detail. You have spent so much time making this CV that you are the worst one to spot any remaining errors. At the very least give it to someone you trust to go over it thoroughly. Ask them to identify any errors for you. And ask them to also let you know if it makes sense and reads as authentic. If you want to spend some additional dollars on it. You can pay someone to review your CV for you.
Many doctors from India have successfully migrated to work in Australia. Doctors from India were the fourth-highest country to be granted a visa to work as a doctor in Australia in 2017. After the United Kingdom, the Republic of Ireland and Malaysia. As someone who has worked in Medical HR for more than two decades, I have found Indian doctors on the whole to be a really good group of doctors to work with.
Can Indian doctors work in Australia? The answer is, of course, yes. India provides one of the largest sources of overseas doctors or International Medical Graduates (IMGs) working in Australia at both a trainee doctor as well as specialist level. Of course, no doctor coming from another country is absolutely guaranteed to be able to work in Australia.
Just like doctors from other countries. Doctors from India are limited in regards to what doctor jobs they can initially apply for in Australia. Once employed you receive the same rates of salary and pay as other doctors, with some possible restrictions on where you can work. Salary packages vary from about $70,000 AUD for a very junior level job to $300,000 AUD and much more for consultant-type positions. There are two main ways that Indian doctors need to either apply for initial registration. Both are quite hard.
The Standard Pathway is the process if you are not a specialist. It requires sitting for the Australian Medical Council exams, which have an overall pass rate of about 60% for the MCQ component and 25% for the clinical component.
The Specialist Pathway is the process if you are a specialist. Between the years 2015 and 2021, 729 specialist Indian doctors applied to a specialist medical college for assessment. 244 were deemed to not be comparable. 401 were deemed to be partially comparable and only 84 were deemed to be substantially comparable (a 66% rate of being found comparable.
So the prospects for working in Australia as an Indian doctor are good for many but challenging for some. So it’s important to give you a little bit more detail. There are also other options for getting registered which I will outline.
So let’s dig into a bit more of the details of the top of Indian Doctors Australia.
Get a Guide
A bundle of resources written by a local Australian expert covering how Indian doctors can work in Australia.
The Standard Pathway. The Option for Trainee Indian Doctors Australia.
If you are a trainee doctor from India and do not have specialty status then the Standard Pathway is the main option for you.
The major hurdle in this process is pursuing the Australian Medical Council examinations, which we have written about in more depth here.
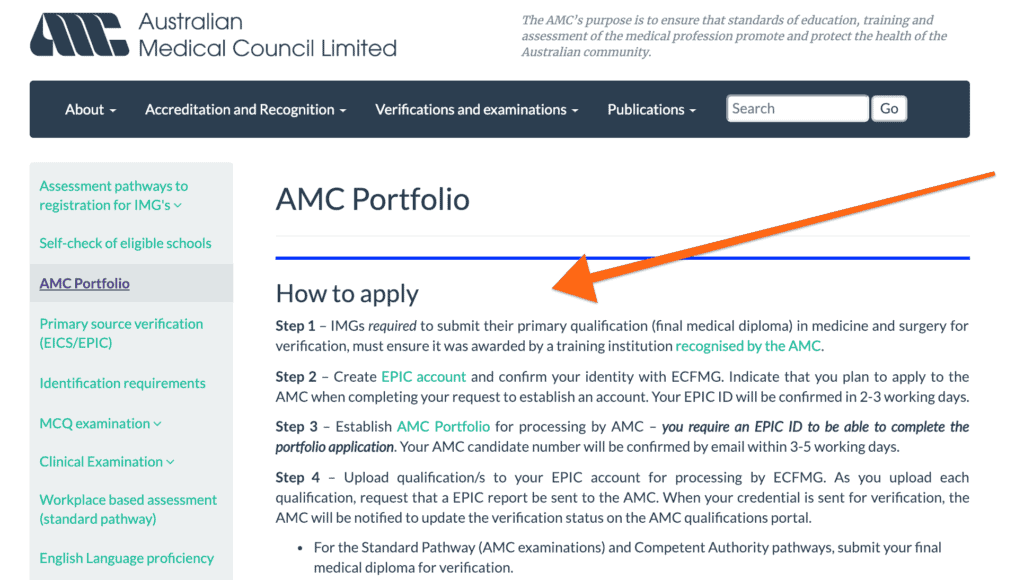
In order to be able to sit for the AMC, you must first establish what is called a portfolio
You first create a registration with the AMC website.
You should also check that your medical degree is awarded by an institution recognized by the AMC. The AMC recognizes most but not all medical schools which are listed with the World Directory of Medical Schools. There is a handy search on the AMC site.
You must then also create an EPIC account and confirm your identity with the ECFMG (located in the United States).
You get an EPIC id in about 3 working days, which you use to establish your AMC portfolio.
You upload your qualifications to EPIC. As you do so YOU MUST REQUEST that EPIC send a report to the AMC.
EPIC notifies you and the AMC when they have completed their check.
This whole process will cost you $500 AUD to register with the AMC and about $205 USD for EPIC (more if you are wanting more than one qualification verified).
Once EPIC reports back in the affirmative to the AMC you will be allowed to request to sit for the AMC Part 1 Examinations.
There is no actual work experience requirement to sit the AMC Part 1 Examination and you can, in fact, start preparing for this whenever you like. But of course, you will not be able to sit the exam without a verified medical degree. So you can start studying for it in medical school but won’t be able to sit it till after you graduate.
The Part 1 MCQ Examination
The AMC Computer Adaptive Test (CAT) MCQ Examination is a computer-administered fully integrated multi-choice question examination delivered in one sitting that lasts 3 and a half hours.
There are regular invigilated examinations in Australia as well as a number of sessions available in the examination across the world.
The examination itself consists of 150 “A-type MCQs”. You must select the one correct response from amongst the five options. 120 of the questions are “live” questions, which means they count towards your score. The remaining 30 questions are being piloted and don’t count towards your final score. You do not know which questions are being piloted so you have to give your best for all 150.
You are expected to complete all 150 items and must complete the 120 scored items. Failure to complete all 120 scored items in the examination may lead to insufficient information for a reliable determination of your ability and therefore a result on the AMC adaptive scale.
You should practice as many MCQs as you can. There is also an official online practice exam through the AMC website.
Because the MCQ exam is computerized you will receive your result fairly quickly in about 4 weeks. You get a printout that indicates where you performed overall, as well as the range for all candidates appearing for that particular exam. You also get a breakdown of your performance in the question domains. This is useful if you don’t pass to know where to put your efforts next time.
You need to score 250 or more to pass. Less than 60% of candidates pass. Although this score is probably depressed somewhat by those candidates sitting more than once.
It currently costs $2,920 AUD to sit for the MCQ.
The AMC Clinical Examination Part 2
Once you pass the AMC MCQ exam, you are then able to appear for the AMC Clinical exam. These are all held in Melbourne at the AMC’s purpose-built examination National Testing Centre or online.
Clinical Exam Format
The Clinical exam format is a 20-station multidisciplinary structured clinical exam that assesses your skills in Medicine, Surgery, Gynecology and Obstetrics, Pediatrics, and Psychiatry. There are 14 scored stations, 2 pilot (non-scored) stations and 4 rest (non-scored) stations.
As of 2019, the result is graded as either a clear pass or a clear fail. Prior to this borderline candidates were offered a retest. However, the AMC found that the time between examination and retest was becoming so long that the results were not meaningful.
You must pass 10 or more of the stations to pass the exam. The pass rate is incredibly low. About 28%
It is recommended that you should study the Handbook of Clinical Assessment and practice roleplays as much as you can. You may want to attend a course. Candidates also study different notes such as Karen notes, and the VMPF notes. John Murtagh’s General Practice is also worth revising.
It is extremely wise to form a study group and there are many groups around where you can practice what is called “recalls”, which is when a candidate who has previously sat the exam attempts to reconstruct the station.
The cost of sitting the Clinical Examination is currently $3,730 AUD ($400 extra for the online version).
When and What types of jobs can I apply for as an Indian Trainee?
You can apply for a range of trainee jobs. The main limitation is whether the employer will accept an IMG. Which for the majority of cases they will not.
You can actually start applying for jobs after you have passed your AMC Part 1 Examination. But you will need a valid English language test if you do.
There are often a number of postgraduate year 2 or 3 general jobs on offer. They are generally termed Resident Medical Officers in most States and Territories, but may also be called House Officers or Hospital Medical Officers in some places.
Above these sorts of posts, come the specialty training positions. In Australia, you tend to enter specialty training around postgraduate year 3. These positions are generally referred to as Registrar positions. But you might also see advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most of these jobs will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice, the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
your previous experience, especially in the type of position for which you have applied
whether you have practised recently and the scope of your recent practice
the requirements of the position including the type of skills required for the position
the position itself, including the level of risk, the location of the hospital or practice and the availability of supports (supervisors)
the seniority of the position, for a hospital position
In general, you will either be approved for Level 1 or Level 2 Supervision. There are 4 Levels and the higher up you go the less direct oversight you require.
Level 1 Supervision.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times and you must consult with them about all patients. This is the level of supervision that most Indian doctors will receive Remote supervision (e.g. by telephone) is not permitted. This type of supervision is generally recommended when you are very junior yourself or entering a junior role which you are not very familiar with. In Australian major public hospitals, there are many layers of other doctors who you can get supervision from. So Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision.
Level 2 Supervision, is what most other Indian trainees approved to work in Australia will be approved for. It is a step up from Level 1 Supervision. Supervision must primarily be in person but your supervisor can leave you to do work on your own and you can discuss it by phone. You should discuss with them on a regular (daily) basis what you have been doing with patients. But do not need to discuss every case.
Level 3 Supervision.
Level 3 Supervision, is what you might receive if you are working in an Advanced Trainee role in India and transferring to something similar in Australia. In this case, you have much more primary responsibility for the patient. Your supervisor needs to make regular contact with you but can be working elsewhere and available by phone or video.
What happens after I commence my position?
Once you are approved for registration and you have your visa issues sorted you will be able to commence work. Your employer should help you out with all these things. You will be working under what is called “provisional registration” by the Medical Board of Australia. Generally, all you need to do for these 12 months is to show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia and it is your responsibility, not theirs to see that they are completed and returned on time. If all the reports go well you will be able to be recommended at the end of the 12 months for general registration.
The other thing that you need to watch out for is that your employer is ensuring that you gain exposure to the types of experiences that the Medical Board requires for this year. Generally, these shadow the experience that Australian interns go through.
Depending on whether you have completed AMC Part 2 or not. You will need to try and sit and pass this in these 12 months. Although you may be able to get an extension.
If you are lucky enough you may be employed in one of the 20 or so health services which offer Workplace-based assessment as an alternative to the AMC Clinical exam. Candidates find this process far easier to complete.
You will probably be starting to look for another job or negotiating an extension around the end of your 12 months. With general registration, you may be able to apply for a skilled visa, as well as be looking at applying for permanent residency.
Permanent residency is crucial for applying for most specialty training programs. See below.
The Specialist Pathway. The Option For Specialist Indian Doctors Australia.
For Indian specialists, your option for working in Australia is what is called the Specialist Pathway.
Once again this starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need position, in which case the employer or recruitment agent will provide you with a lot of support and will likely pick up the costs of being assessed.
For most International Doctor specialists however these days you will be approaching the college directly to be assessed for specialist recognition. This is not something to be trifled with. The paperwork requirements and the cost (generally around $10,000 AUD or more) is considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
Finding Out What You Need To Do.
We have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The majority of Indian specialties (but not all) map to a similar college or specialty in Australia. So working out which specialty goes into which Australian college is generally not too confusing. We have put together a summary of the Australian specialist medical colleges here.
After you go through your specialist assessment you are given an outcome.
As I have noted the majority of cases for Indian specialists are either deemed not comparable or substantially comparable.
If you are deemed not to be comparable by the college. This means you cannot directly become a specialist in Australia. You will probably have to go through the standard pathway to work as a doctor in Australia.
If you are deemed to be partially comparable (a situation where this commonly may occur is if you have just recently finished specialty training but have not worked as a specialist for very long). In this situation you will need to work under supervision for longer and may well also face some formal examinations.
Substantially comparable is the best result. This essentially means that you will need to work under some form of peer review for up to 12 months and so long as your reports are satisfactory you will be recommended for specialist registration at the end.
How to Maximize Your Chances of Getting a Substantially Comparable Outcome.
To ensure that you are seen as substantially comparable by the relevant college I would recommend the following:
You should have your Certificate of Completion of Training and relevant college Fellowship
You should ideally have worked substantively at a Consultant level in your field for 3 years or more
You should be able to demonstrate good standing with your Medical Board and your employers
You should be able to demonstrate ongoing continuing professional development
You should prepare for your interview with the college as if it were an important job interview
Can you enter training in Australia if you are an Indian doctor?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in some cases permanent residency or citizenship.
After receiving your general registration you can apply for specialty training in the same way that Australian-trained doctors do. And if accepted will go through the exact training program and experience. Some colleges may offer recognition of prior learning for any training you have done already. But this is often quite limited and may at best normally shave one year off of your training.
An Alternative But Limited Option.
There is an alternative but time-limited pathway for Indian doctors who are just seeking a short-term experience in Australia to add to their training in India. This is called the Short-Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in India or be less than two years from completion. So this is a program mainly for early career specialists or advanced trainees.
In this pathway you go through the same steps with the AMC as per the competent authority pathway to gain registration. You will not, however, be able to apply for specialist assessment as part of this pathway. But if you gain general registration you may then be able to apply for another position and then apply for specialist assessment.
Can you do your internship in Australia as an Indian doctor?
Basically no. Internship in Australia is a provisional year that only applies to medical graduates from medical schools in Australia and New Zealand. There is a “loophole” which only applies to doctors who have not been able to complete an internship or equivalent in their own country. But the Medical Board warns that this is not a great option and is only granted in limited cases. You are far better off completing the requirements for general registration in India.
How many Indian doctors are working in Australia?
There is no one public data source to tell us how many Indian doctors are currently working in Australia.
From data collected by the Australian Government, we know that:
171 working visas were granted to Indian doctors to work in Australia in the year 2017.
729 applications were made for specialist assessment, of which 244 were deemed not comparable, 401 partially comparable and only 84 substantially comparable (2015-2021).
How hard is it to become a specialist in Australia if you are from India?
As we have noted. Many Indian doctors struggle to gain recognition as a specialist. This normally occurs in the first step. The initial specialist college assessment. Once Indian doctors are granted comparability. Most go on to complete the process.
Are there any particular specialties that are easier to apply for?
The majority of specialties have some vacancies and will provide opportunities for Indian and other IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be quite difficult.
On the other end of the spectrum general practice, psychiatry and most parts of critical care medicine are often always looking for doctors.
Costs of Moving To Australia and Working As a Doctor.
There are lots of costs to consider when thinking about moving to Australia to work as a doctor.
There are some direct costs to consider. Most of which relate to the bureaucratic process of being assessed and gaining registration.
Some of the costs you may be up for, include:
AUD (unless otherwise noted)
Establish a Portfolio with the Australian Medical Council
$600
Registering with EPIC and having one primary degree checked
$125 USD + $80 USD
Medical Board Application Fee for Provisional Registration
$430
Medical Board Application Fee for Specialist or General Registration
$860
College Specialist Assessment Fees
$6,000-$11,000
College Placement Fees (for the period of supervision)
$8,000-$24,000
Further, if you are required to undertake further exams there will be a cost for this as well. As an example, RACS charges exam fee is $8,495.
The Cost of Your Time and Effort.
Adding to all of this financial cost, you will need to factor in the cost of your own time. It takes a lot of effort and persistence to deal with the paperwork and track down the records you need.
In addition, you are probably going to have to pay costs in your own country for things like records of schooling and certificates of good standing.
There are also visa costs.
And then there is the cost of airfares and transporting your belongings halfway across the world.
Depending on where you work in Australia you may find that the cost of living is higher or lower than you are used to. House prices and therefore house rental rates have gone through the roof in Australia in the last decade or so but are starting to come down.
You will probably have to factor in some initial extra hotel or short-term rental charges whilst settling in and you may find if you have children that you have to pay to enrol them in school as public schooling is only generally free if you are a citizen or permanent resident.
If you are lucky and in one of the specialty areas of demand your employer may offer to pay for some of these costs. It’s certainly worth asking about it.
The Competent Authority Pathway. An Option For Some Indian Doctors.
If you have already worked in the United Kingdom, Canada or the United States then you may be able to apply to work in Australia under what is called the competent authority pathway.
The competent authority pathway assigns a preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States and the Republic of Ireland.
There is largely an historical rationale for this situation. It is based on the premise that all these jurisdictions have similar approaches to medical school training and similar standards.
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools, the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically to those from Australia.
If you are an international medical graduate and you have achieved general registration in the United States, Canada or the United Kingdom (but not the Republic of Ireland) you are also eligible for the competent authority pathway.
What are the steps involved for the competent authority pathway?
Applying to the Australian Medical Council for primary source verification
Applying for registration to the Medical Board of Australia
Completing 12 months of supervised practice
Applying again to the Medical Board of Australia for general registration.
Eligibility for Competent Authority
You can do a “self-assessment of your eligibility for the competent authority pathway on the Medical Board of Australia website here.
The essential requirements for Indian doctors applying via the competent authority pathway are:
You need to have completed the appropriate process in Canada, the United States or the United Kingdom to become fully registered in that country. This involves an assessment of your English language skills, examinations and a period of supervised training.
So for example, if you have worked in the United Kingdom, you need to successfully complete the Professional and Linguistic Assessments Board (PLAB) test
AND
Successfully complete the Foundation Year 1, or 12 months supervised training (internship equivalent) in the United Kingdom, or 12 months supervised training (internship equivalent) completed in another Medical Board Australia approved competent authority country, approved by the GMC.
Conclusion.
We hope that you found this summary about how Indian doctors can work in Australia useful. If you have any questions or queries or just want to relate your experience. Please feel free to leave a comment below. We would love to hear from Indian doctors who have made the journey to Australia.
Related Questions.
Question: Are there any other options for working as an Indian doctor in Australia?
Answer. Some doctors just want to come to Australia for a limited period of time as an opportunity to train in another country. As we have highlighted above there is an alternative but time-limited pathway for Indian doctors who are just seeking a short-term experience in Australia to add to their training in India. This is called the Short-Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in India or be less than two years from completion. So this is a program mainly for early career specialists or advanced trainees.
Question: Should I use a medical recruitment company if I am considering working in Australia?
Answer. It is possible to deal directly with employers in Australia as an Indian doctor. In general, however, when moving from one country to another most doctors find it useful to engage with a medical recruitment company as they can tend to take some of the stress out of the planning for you and help with all the paperwork and negotiating with prospective employers. Some medical recruitment companies also provide migration services and relocation services as well. We have written more on this subject here. And a list of medical recruitment companies is available here. Unfortunately, for most Indian doctors medical recruitment companies will be unlikely to be able to help you until you have either achieved general registration via the Standard Pathway or possibly until you have received a favourable outcome via the specialist pathway process. See more about the pros and cons of medical recruitment companies here.
Your referees and job references are arguably the most important aspect of your CV or Resume. It is important to carefully consider who you choose to speak on your behalf. Some employers look for recognisable names or organisations in your referee list. This is why referees are always listed last on your CV or resume.
Should you list job references on your CV as a Doctor? The answer is yes. In medical applications it is expected that you will list referees. You should list them as the very last item on your CV. The employer will generally not proceed to offer you an interview without them. In regards to who to choose.
You are normally requested to list 3 referees. So it is generally recommended that at least one of these be a current or recent supervisor (last 6 months). One should be someone senior within the specialty you are applying (preferably a consultant). Your final referee should be someone different from the previous two. This is in order to display your diversity and ability to make good connections in your work teams.
It’s a lot more complex than this. For example, often your recent supervisor is also a Consultant. And you can sometimes list more than 3 referees. So I’m going to explain things in a bit more detail, including how who and when to approach referees, how to keep them updated and conclude with a recommendation as to how you list your referees on your CV.
Referee Choice.
So. Who are the best people to choose for job references? Most job applications these days are online and in the online, eRecruitment systems you generally have the opportunity to list 3 up to referees. However, you often do not have a complete choice in who you list.
Many prospective future employers will ask for you to list at least one referee who is your current supervisor or manager. Or at the very minimum a recent supervisor. If you are opting for a recent supervisor try to include someone who was supervising you in the past 6 months.
Why do they want to speak to a recent supervisor? The reason is simple. The employer wants to check on your current performance. Sometimes candidates list supervisors that they worked for several years ago who can give quite glowing appraisals. The problem is the same candidate has had a series of bad job outcomes in more recent times.
Actually, it is generally sensible to have at least 2 of your referees be current or recent supervisors. That way there can be no doubt from the employer that you are genuine about your recent work history and very happy for them to contact the people they want to contact.
The Final Slot.
You should try to reserve the third slot for someone who helps you demonstrates the diversity of your connections and is different from your other two referees.
For example, if both your supervisor referees are late middle-aged male consultant orthopaedic surgeons, then being able to list a female colleague from another department or even another profession would be a distinct advantage.
Whilst the online recruitment systems will generally limit you to 3 referees. There is no reason why you cannot list more than three on your CV or resume if you think this helps your application. But be sure that you are listing the same top 3 referees in the same order on your application as your CV.
The Importance Of References
The reason why job references on doctor CVs are listed last is to make them easier to find. Most employers when reviewing your CV for the first time will only take a few seconds to consider it. They will quickly review the short details on your front page, note your name, scan your personal or career statement and check out what recent jobs you have done. They will then flick over to the back to see if they recognise any of your referees or the places that your referees work at. That’s it.
Experienced recruiters know to weigh the value of a well-taken reference or set of references above the quality of your interview performance. This is because studies show that references have greater predictive validity in selection.
Often References Are Poorly Utilized.
Sadly, many of the doctors you will encounter on selection panels do not know this fact and place too much emphasis on the interview performance. But this does not mean that they are not interested in your referees. They are.
Another problem with referees and reference reports is that they are often conducted and collected poorly, particularly in bulk medical recruitment processes.
Sometimes your referees are contacted before your interview (which is better as it avoids confirmation bias) often this is done afterwards. In any case, it is a requirement that your references are taken prior to being offered a position if you are a successful candidate. So, referees both act as evidence of your quality as a candidate as well as a verification that what you have said about yourself is indeed true.
So. Who should I choose for my referees?
As I have already stated in most industries it is expected that your first referee will be your current supervisor or manager and your second referee will generally be your previous supervisor or manager.
Medicine can be a little different particularly for trainee doctors who are rotating around frequently. You are often interacting with several supervisors and managers on a regular basis. So it can be tough to work out exactly who constitutes a current or recent manager or supervisor.
There are three key principles that I outline to trainee doctors when selecting referees to help to make things a bit easier. The first is recency, the second is relevancy and the third is diversity.
There are three key principles that I outline to trainee doctors when selecting referees to help to make things a bit easier. The first is recency, the second is relevancy and the third is diversity.
Dr Anthony Llewellyn | Career Doctor
Recruiters will generally want to speak to someone who has recently worked with you, preferably your current manager. In some circumstances, this is a requirement. If you are a senior medical practitioner its usually fairly obvious who this person is. If you are an intern or a resident or a specialty trainee you actually have quite a range of options all of which will generally be acceptable to the selection panel.
Recent Supervisor Options For Trainee Doctors.
Some good options for trainees might be your Director of Training, Director of Medical Services or Medical Workforce Unit or JMO Manager. You might also consider your Nurse Unit Manager.
As a trainee doctor, you also want at least one referee who is relevant to your chosen career. For most this generally means one Consultant who is a Fellow of the Specialty College you are aiming to enrol with.
Some doctors in training try to have 3 College Fellows listed as their only referees and worry if this is not the case. It can be incredibly hard to collect 3 good referees from one College and I actually don’t recommend this approach. You are far better off focusing on obtaining one College referee who has actually supervised you in a term. Most trainee doctors will have a chance to work one term in their preferred specialty before applying for posts.
Rounding Off Your Referees.
So who else might you ask to act as a referee? This is where diversity is a consideration. There may be a Consultant from another specialty who you got on well with in their term. If so, it’s a good idea to put them down. Other options include: Nurse Managers, Senior Allied Health Professionals, and Advanced Trainees. The key consideration here is that these should be people that you have worked with who have gotten to know you reasonably well.
I would also recommend that at least one of your referees is male and at least one is female.
By having a diverse list of referees you are telling the selection panel that you value teamwork and the roles of others in the team and also that you are able to get on well with and connect with a range of different people in the workplace.
More senior medical practitioners will probably go with their current Supervisor, for e.g. Head of Department and if working in a hospital possibly their Supervisor’s supervisor, for e.g. the Director of Medical Services. They may also then opt to diversify out the final referee by seeking a reference from a peer in another profession, which is generally either a straight out Manager or another health professional in a senior or management role.
Having More Than 3 Referees.
Very occasionally you are asked to list 2 referees but in most cases you are asked for at least 3. There is actually a practical reason for this.
In order to progress you to a job offer, the panel will generally be required to contact at least 2 referees. So this means that if they are contacting your referees after the interview it’s almost generally a good sign. They usually stop at 2. The third referee is there in case one of your other 2 referees are not able to be contacted.
So one of the key things to think about with your referees is are they going to be available at the time that they are likely to be needed. If your referee is attending an overseas conference don’t let this be the thing that stops you from finding out about your application result!
But there is no rule that says you have to stop at 3 referees. You can list more. And it may be sensible to add a couple of more referees in case one or two of the top ones might be hard to contact. You may also feel that additional referees enhance your candidacy further. Extra referees can, for example, demonstrate your ability to be a team player by listing additional referees from a range of areas of medicine and a range of disciplines.
You might also have some academic or research supervisors that you wish to include. Even though the job you are applying for is clinical.
More than 5 or 6 referees on a CV however is probably excessive.
The Order Of Your Referees Is Important.
You should also be mindful of the order in which you list your referees.
Remember that the first two people listed on your CV as a referee are the ones that will be contacted first for a reference. So you should generally order your list of referees in the order that you would prefer them to be contacted. However, if one of your referees is someone you have not worked within over 12 months then you should either rethink using them as a reference or put them a bit further down your list (at 3rd or 4th or 5th spot).
How to Actually Write Up Your Referees.
For online applications, you normally just fill in the boxes as they are ordered. You will probably be asked for your referees’ name, their phone and email contact details and possibly also some information about their working relationship with you.
On your CV or Resume you should list your referees as follows:
Dr Sandy Duncan, Head of Department of Medicine, St Cliffs Hospital, Sydney, 6122 222 222, drduncan@advancemed.com.au
You may wish to add relevant qualifications (e.g. College Fellowship) if this clarifies the nature of the referee better. But you don’t need to list all of their qualifications.
You generally do not need to provide a physical address or postal address.
If possible list a mobile phone number and email address as this helps the person taking a reference.
Approaching Referees and Keeping Them Updated
You should feel free to approach anyone you feel would act as a useful referee.
For trainee doctors, the end of the term is a good time to ask for references. Ask anyone in your team that you are comfortable with if they would be happy to act as a referee for you, i.e. your Consultant, your Registrar, your Nurse Unit Manager. Ask them if it would be ok to use their mobile number and email address. But at this stage, it is generally not useful to ask them to write you a reference. And you should politely decline such an offer if it is made. This may end up being unnecessary.
It is important to keep your referees up to date about your career plans. For anyone you have decided you would like to use as a referee try to keep in reasonably regular contact with them even if it is having a quick coffee with them or dropping them an email.
Coming Up To Recruitment Time.
As you are approaching the recruitment period. Finalise who you are wanting to act as a referees and get in contact with them again. Remind them who you are. Many busy consultants and Nurse Unit Managers see quite a number of medical students and trainee doctors in a year so they may need a bit of a prompt.
Tell them your plans (what you will be applying for and roughly when). Let them know what might be required of them (for e.g. will they have to fill in an electronic reference, will they need to write a letter of reference to the College?).
Once you have completed your CV send it to them in an email so they have something to base their reference on. Some referees can be quite popular and most are quite busy so a quick email summary of your CV and your interactions with them can also be useful.
Related Questions.
Question: Are there some referees I should avoid or seek out?
Answer. As a trainee doctor, in particular, you may be worried that a certain referee may be tougher than another referee or that some referees carry more weight because of their name, reputation, and connections.
There is a small amount of evidence that more junior consultants are likely to give more glowing references than seasoned or experienced consultants.
But really there is no hard and fast way of knowing whether a referee is more or less likely to improve your chances of an interview or successful job application. Gut feel is probably your best ally here. If you feel that you have established a good authentic working relationship with a referee, they are likely to give you a good reference or at worst a balanced one.
Personally, I would avoid any referee that infers that their name on your CV will carry some sort of additional weight.
Question: Is it OK to put down “Referees Available Upon Request”
Answer. Wherever possible you should attempt to list your referees for the selection panel. In some cases, however, there may be some sensitivity around giving out referees, particularly as you progress in seniority. Candidates may sometimes want to speak to the employer first before contacting a referee or they may want to feel that they have a good chance of getting the job before alarming their current employer. In some cases, they may just be having trouble contacting their referee because they are aware. Employers recognise that the words “Referees Available Upon Request” means that the candidate needs to have a conversation first. So its ok to do this if your situation really does call for it.
Any doctor who has worked for more than a few months in Australia will likely have worked alongside a UK doctor who has decided to work in Australia. Whether this is for a short-term working holiday or a permanent move. As someone who has worked in Medical HR for more than two decades, I have found that UK doctors on the whole to be a really good group to work with. So let’s talk about UK Doctors Australia.
Can UK doctors work in Australia? The answer is, of course, yes. The United Kingdom provides the largest source of overseas doctors or International Medical Graduates (IMGs) working in Australia. Of course, no doctor coming from another country is absolutely guaranteed to be able to work in Australia.
But because the UK medical training system is recognized by the Medical Board of Australia as being on par, UK doctors have good success with either becoming generally registered through what is called the competent authority pathway or being recognized as a specialist through the specialist pathway. In 2017 (the latest year we have figures for) 430 UK doctors were recommended for specialist registration, with many more achieving general registration.
So the prospects for working in Australia as a UK doctor are extremely good. But it’s important to give you a little bit more detail. As I have highlighted there are two main options for getting registered. So we will talk about these first and then go into some other common questions.
The Competent Authority Pathway. The Option For Trainee UK Doctors Australia.
If you are a trainee doctor in the UK. Then you are looking at the competent authority pathway for working in Australia.
The competent authority pathway assigns a preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States, and the Republic of Ireland.
There is largely a historical rationale for this situation. It is based on the premise that all these jurisdictions have similar approaches to medical school training and similar standards.
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools, the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically as those from Australia.
If you are an international medical graduate and you have achieved general registration in the United States, Canada, or the United Kingdom (but not the Republic of Ireland) you are also eligible for the competent authority pathway.
What are the steps involved for the competent authority pathway.
Applying to the Australian Medical Council for primary source verification
Applying for registration to the Medical Board of Australia
Completing 12 months supervised practice
Applying again to the Medical Board of Australia for general registration.
Eligibility for Competent Authority
You can do a “self-assessment of your eligibility for the competent authority pathway on the Medical Board of Australia website here.
The essential requirements are:
You need to be a graduate of a medical course conducted by a medical school in the United Kingdom which is accredited by the General Medical Council
AND
Successfully complete Foundation Year 1, or complete 12 months supervised training (internship equivalent) in the United Kingdom, or complete 12 months supervised training (internship equivalent) another Medical Board of Australia approved competent authority country, which is also approved by the GMC.
OR if you are an IMG who has been working in the United Kingdom you need to
Successfully complete the Professional and Linguistic Assessments Board (PLAB) test
AND
Successfully complete the Foundation Year 1, or 12 months supervised training (internship equivalent) in the United Kingdom, or 12 months supervised training (internship equivalent) completed in another Medical Board Australia approved competent authority country, approved by the GMC.
For this reason, doctors who have completed medical school in another European Union country are often unable to get registered in Australia via working in the United Kingdom as they are often not required to complete the PLAB.
What types of jobs can I apply for as a UK Trainee?
You can pretty much apply for any sort of trainee job. There are often a number of postgraduate year 2 or 3 general jobs on offer. They are generally termed Resident Medical Officer in most States and Territories, but may also be called House Officer or Hospital Medical Officer in some places.
Above these sorts of posts, come the specialty training positions. Australia’s specialty training system is fairly much in parallel with the United Kingdom. So you tend to enter specialty training around postgraduate year 3. These positions are generally referred to as Registrar positions. But you might also see advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most of these jobs will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice, the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
your previous experience, especially in the type of position for which you have applied
whether you have practiced recently and the scope of your recent practice
the requirements of the position including the type of skills required for the position
the position itself, including the level of risk, the location of the hospital or practice and the availability of supports (supervisors)
the seniority of the position, for hospital position
In general, you will either be approved for Level 1 or Level 2 Supervision. There are 4 Levels and the higher up you go the less direct oversight you require.
Level 1 Supervision.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times and you must consult with them about all patients. Remote supervision (for e.g. by telephone) is not permitted. This type of supervision is generally recommended when you are very junior yourself or entering a junior role with which you are not very familiar with. In Australian major public hospitals, there are many layers of other doctors from who you can get supervision from. So Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision.
Level 2 Supervision, which is what most UK trainees approved to work in Australia will normally be approved for is a step up from Level 1 Supervision. Supervision must primarily be in person but your supervisor can leave you to do work on your own and you can discuss by phone. You should discuss with them on a regular (daily) basis what you have been doing with patients. But do not need to discuss every case.
Level 3 Supervision.
Level 3 Supervision, is what you might receive if you are working in an Advanced Trainee role in the UK and transferring to something similar in Australia. In this case, you have much more primary responsibility for the patient. Your supervisor needs to make regular contact with you but can be working elsewhere and available by phone or video.
What happens after I commence my position?
Once you are approved for registration and you have your visa issues sorted you will be able to commence work. Generally, your employer helps you out with all these things. You will be working under what is called “provisional registration” by the Medical Board of Australia.
Generally, all you need to do for these 12 months is to pay attention, show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia and it is your responsibility, not theirs to see that they are completed and returned on time. If all the reports go well you will be able to be recommended at the end of the 12 months for general registration.
You will probably be starting to look for another job or negotiating an extension around this time. With general registration, you may be able to apply for a skilled visa, as well as be looking at applying for permanent residency.
Permanent residency is crucial for applying for most specialty training programs. See below.
The Specialist Pathway. The Option For UK Specialists
For UK specialists your option for working in Australia is what is called the Specialist Pathway.
Once again this starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need position, in which case the employer or recruitment agent will provide you a lot of support and will likely pick up the costs of being assessed.
For most International Doctor specialists however these days you will be approaching the college directly to be assessed for specialist recognition. This is not something to be trifled with. The paperwork requirements and the cost (generally around $10,000 AUD or more) are considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
Finding Out What You Need To Do.
We have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The majority of UK specialties (but not all) map to a similar college or specialty in Australia. So working out which specialty goes into which Australian college is generally not too confusing. We have put together a summary of the Australian specialist medical colleges here.
After you go through your specialist assessment you are given an outcome.
In the majority of cases for UK specialists, you will be deemed substantially comparable. This essentially means that you will need to work under some form of peer review for up to 12 months and so long as your reports are satisfactory you will be recommended for specialist registration at the end.
Occasionally UK specialists are deemed to be partially comparable (a situation where this may occur is if you have just recently finished specialty training but have not worked as a specialist for very long). In this situation, you will need to work under supervision for longer and may well also face some formal examinations.
Rarely are UK specialists deemed not to be comparable by the college. This only happened to 6 out of 409 UK doctors in 2017 (less than 1%). If you are deemed to be not comparable, this means you cannot directly become a specialist in Australia. You will probably have to go through the competent authority route and re-enter training in Australia.
How to Maximize Your Chances of Getting a Substantially Comparable Outcome.
To ensure that you are seen as substantially comparable by the relevant college I would recommend the following:
You should have your Certificate of Completion of Training and relevant college Fellowship
You should ideally have worked substantively at a Consultant level in your field for 3 years or more
You should be able to demonstrate good standing with the GMC and your employers
You should be able to demonstrate ongoing continuing professional development
You should prepare for your interview with the college as if it were an important job interview
Can you enter training in Australia if you are a UK doctor?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in many cases permanent residency or citizenship.
After receiving your general registration UK doctors can apply for specialty training in the same way that Australian trained doctors do. And if accepted will go through the exact training program and experience. Some colleges may offer recognition of prior learning for any UK training you have done already. But this is often quite limited and may at best normally shave one year off of your training.
An Alternative But Limited Option.
There is an alternative but time-limited pathway for UK doctors who are just seeking a short-term experience in Australia to add to their training in the UK. This is called the Short Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed your training in the UK or be less than two years from completion. So this is a program mainly for early-career specialists or advanced trainees.
In this pathway, you go through the same steps with the AMC as per the competent authority pathway to gain registration. You will not, however, be able to apply for specialist assessment as part of this pathway. But if you gain general registration you may then be able to apply for another position and then apply for specialist assessment.
Can you do your internship in Australia as a UK doctor?
Basically no. Internship in Australia is a provisional year that only applies to medical graduates from medical schools in Australia and New Zealand. There is a “loophole” that only applies to doctors who have not been able to complete an internship or equivalent in their own country. But the Medical Board warns that this is not a great option and is only granted in limited cases. You are far better off applying for the Foundation Program in the UK and completing at least Foundation Year 1.
How many UK doctors are working in Australia?
There is no one public data source to tell us how many UK doctors are currently working in Australia.
From data collected by the Australian Government, we know that for 2017 (latest available year):
718 applications were made for provisional registration via the competent authority pathway by UK doctors with 701 granted provisional registration
An additional 43 applications were made for provisional registration via the competent authority pathway by doctors who had completed the PLAB in the UK, with 31 being granted provisional registration
409 applications were made for specialist assessment, only 6 of which were deemed not comparable, 36 partially comparable and 367 substantially comparable.
430 UK doctors were recommended for specialist recognition with 12 not being recommended
How hard is it to become a specialist in Australia if you are from the UK?
Specialist doctors from the United Kingdom are not automatically granted specialist recognition. However, most are. As you can see from above in 2017 there were 409 applications made for specialist assessment to the Australian colleges by UK doctors and of these, the majority were deemed substantially comparable.
UK doctors tend to get a very favourable outcome in comparison to doctors from most other countries. The UK has generally the highest rate for doctors being seen as substantially comparable. Even when comparing to the other competent authority countries of the United States, Canada and the Republic of Ireland.
We hope that you found this summary about how UK doctors can work in Australia useful. If you have any questions or queries or just want to relate your experience. Please feel free to leave a comment below. We would love to hear from UK doctors who have made the journey to Australia.
Are there any particular specialties that are easier to apply for?
The majority of specialties have some vacancies and will provide opportunities for the UK and other IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be quite difficult.
On the other end of the spectrum general practice, psychiatry and most parts of critical care medicine are often always looking for doctors.
Costs of Moving To Australia and Working As a Doctor.
There are lots of costs to consider when thinking about moving to Australia to work as a doctor.
There are some direct costs to consider. Most of which relate to the bureaucratic process of being assessed and gaining registration.
Some of the costs you may be up for, include:
AUD (unless otherwise noted)
Establish Portfolio with Australian Medical Council
$500
Registering with EPIC and having one primary degree checked
$125 USD + $80 USD
Medical Board Application Fee for Provisional Registration
$382
Medical Board Application Fee for Specialist or General Registration
$764
Medical Board Provisional Registration Fee
$382
Medical Board General or Specialist Registration Fee
$764
College Specialist Assessment Fees
$6,000-$11,000
College Placement Fees (for a period of supervision)
$8,000-$24,000
Further, if you are required to undertake further exams there will be a cost for this as well. As an example, RACS charges an exam fee is $8,495.
The Cost of Your Time and Effort.
To all of this cost, you will need to factor in the cost of your own time. It takes a lot of effort and persistence to deal with the paperwork and track down the records you need.
In addition, you are probably going to have to pay costs in your own country for things like records of schooling and certificates of good standing.
There are also visa costs.
And then there is the cost of airfares and transporting your belongings halfway across the world.
Depending on where you work in Australia you may find that the cost of living is higher or lower than you are used to. House prices and therefore house rental rates have gone through the roof in Australia in the last decade or so but are starting to come down.
You will probably have to factor in some initial extra hotel or short-term rental charges whilst settling in and you may find if you have children that you have to pay to enroll them in school as public schooling is only generally free if you are a citizen or permanent resident.
If you are lucky and in one of the specialty areas of demand your employer may offer to pay for some of these costs. It’s certainly worth asking about it.
Related Questions.
Question: Are there any other options for working as a UK doctor in Australia?
Answer. The Competent Authority Pathway and the Specialist Pathway are the only two pathways for UK doctors to work in Australia.
Question: Should I use a medical recruitment company if I am considering working in Australia?
Answer. It is possible to deal directly with employers in Australia as a UK doctor. In general, however, when moving from one country to another most doctors find it useful to engage with a medical recruitment company as they can tend to take some of the stress out of the planning for you and help with all the paperwork and negotiating with prospective employers. Some medical recruitment companies also provide migration services and relocation services as well. We have written more on this subject here. And a list of medical recruitment companies is available here.
A question I am often asked by other doctors is when is a medical recruitment agency a good idea. Not surprisingly when you google this topic you get a list of articles written by medical recruitment agencies so I felt it would be useful to add an independent perspective.
Some of the key reasons you may want to use a medical recruitment agency, also known as a locum company, include:
obtaining short term work (otherwise known as locum work), recruitment agencies are adept at filling gaps in hospital rosters and negotiating better rates on your behalf;
to gain access to a more extensive list of permanent roles and opportunities, recruitment agents can help to cut down your own effort in the job search; and
to help you find a doctor job opportunities in another location, for example relocating to another country, many recruitment agents will provide a comprehensive set of services that include assisting with obtaining the job, handling the regulatory and visa paperwork and even relocation services.
A quick reminder that if you are considering working with a medical recruitment agency. We do appreciate if you reach out to AdvanceMed first as we will be able to guide you. And if it does make sense to work with a medical recruitment agency, AdvanceMed may receive a referral fee, which helps us to continue to produce free content, such as this blog post.
So what are the circumstances where you would probably not wish to use a recruitment agency? Let’s examine these before going into more detail about the advantages of recruitment agencies.
When Is It Not Helpful To Use a Medical Recruitment Agent?
The simple answer to the above question is to consider the economic concept of supply and demand. Medical Recruitment Agencies are companies that specialise in finding candidates for hospitals and health services. They are normally called upon when the hospital and health service has exhausted all its usual recruitment strategies and tactics. There is one particular exception to this which will discuss shortly.
But for the most part, you can now see the sorts of scenarios where a recruitment agency can be useful to a hospital or health service and therefore also a smart move for the doctor themselves.
If, however, the hospital or health service is not having difficulty attracting candidates for jobs then it is generally not useful to go through a medical recruitment agent. And, in fact, it can possibly hurt your chances.
Let me explain.
If, as is often the case, a hospital advertises a post for a basic unaccredited surgical trainee role for 6-months as part of an activity to cover a gap in its roster of trainees. Then that hospital is likely to get a number of applications, including from trainee doctors already working in the hospital who are keen to get their first job working in surgery. If you apply for this job via an agency it will cost the hospital an additional premium on top of your wages to hire you. Because this is how recruitment agencies make money. So it’s likely that you might be overlooked for an interview just because of this.
So the sorts of situations where its wiser to apply directly to hospitals and health services in Australia, include:
Applying for general entry level jobs, such as Resident Medical Officer and House Officer roles, particularly if you are an International Medical Graduate, as you will be competing against a number of other candidates;
Jobs you are already aware of in your local network; and
Jobs you have already been invited to apply for.
As indicated above. Some International Medical Graduates, in particular, will find that medical recruitment agencies may either be unwilling to accept them or provide little support. Particularly, if you are going via the standard pathway to registration. You can see that this makes business sense from the medical recruitment agency. The odds of successfully placing an IMG who has the AMC Part 1 exam and no permanent residency or citizenship are extremely low.
Similarly, many Specialist IMGs (SIMGs) may find that medical recruitment agencies are unable to help or support until after you receive a favourable college specialist assessment.
What Sort Of IMGs Are The Medical Recruitment Agencies In Australia Interested In?
You can best tell what sort of IMGs the recruitment agencies in Australia are interested in by looking at the types of jobs that they advertise.
It basically boils down to three key criteria:
what area of medicine you would like to work in;
what country you have trained in; and
where you are prepared to work.
Areas of Medicine That Often Require IMGs
There are generally always gaps in most areas of medicine in a country like Australia, particularly in rural or regional areas. Areas such as general practice, psychiatry, and emergency or critical care medicine are often in high demand for additional staff. This is because there is quite a high demand for these specialties and this demand often outstrips their popularity amongst doctors.
As a broad rule the more “general” you are in your skills or interests as a doctor the more likely you are to find employment. As an example, a general physician is likely to have many more opportunities than a cardiologist. And a general surgeon has more opportunities than a cardiothoracic surgeon.
In addition specialties and subspecialties where procedures are performed generally have an oversupply of doctors in Australia. This partly reflects a similar situation in other countries. But also partly reflects that the remuneration available for performing procedures outstrips consulting activities.
Preferred Countries
Medical Recruitment Agencies will prefer to work with doctor candidates from the following countries:
New Zealand
United Kingdom
Republic of Ireland
United States of America
Canada
Doctors from New Zealand have almost the same status as Australia and can easily obtain registration. Doctors from the UK, Republic of Ireland, US, and Canada are able to more easily gain general registration through the competent authority process. Specialists from these countries also find that they are more easily able to progress through the specialist registration process.
As an example, doctors from the UK dominate the number of doctors who apply for specialist registration each year. In 2017 252 UK doctors out of a total of 309 doctors applied for special recognition as a GP. We don’t know how many were deemed comparable in General Practice but we do know that overall 99% of UK doctors who applied for specialist recognition were deemed either partial or substantially comparable. With 89% being deemed substantially comparable.
So, as a medical recruitment agency, armed with that knowledge you will obviously see a UK doctor as a “good bet” to gain registration and therefore worth working with.
Where Are You Prepared To Work?
The other consideration taken into account is where you would like to work in Australia. The highest proportion of vacancies for medical jobs is generally the inverse of where the population centers are. So if you are prepared to work in remote and rural areas you are likely to have several employers interested in you. Whereas, if you want to work in the heart of Sydney you are going to struggle.
So the ideal IMG candidate from a recruitment agency would probably be an experienced General Practitioner from the United Kingdom looking to relocate to Australia to a small town for family and lifestyle reasons.
And the ideal non-candidate from a recruitment agency would probably be an IMG with only a primary medical degree, from a non-competent authority country, who has passed AMC Part 1 (but not 2) and is only prepared to work in a capital city.
Using Medical Recruitment Agencies For Locum (Short Term) Work
We have spent a fair bit of time so far talking about International Medical Graduates and medical recruitment agencies but of course, medical recruitment agencies also work with doctors with established qualifications and registration in Australia.
Working short term jobs is generally referred to as doing a “locum”, which comes from the Latin locum tenens, a phrase that means “to hold the place of, to substitute for.”
This can be a great option for both trainee doctors as well as specialist doctors. Some of the advantages of locumming include:
you are generally paid at a much higher rate than if you are working for the hospital or service that you are filling in for;
you can take breaks between locum shifts to do other things like study or go on a holiday;
you can select between opportunities;
you can try out different jobs and different places.
Possibly one of the best reasons I have seen for doctors to do a locum is when they have just completed their specialist training and are wanting to try out different locations and services where they might want to take up a more permanent position.
But there are also potential downsides to locumming. Firstly, whilst you can to some extent pick and choose what you do. If you are too choosy then you might start to not get offered any shifts. Secondly, the types of locum jobs on offer might not exactly be in the field of medicine you want to practice and you might have to take on other roles. Thirdly, with extra pay also generally comes the expectation that you are able to work at a higher capacity and level of responsibility with very little orientation or training and this might push you past your comfort zone. Finally, if you are a trainee doctor locumming then you will have to consider how you prove to the Medical Board that you have been maintaining your professional development.
Using Medical Recruitment Agencies To Expand Your Access To Jobs
Medical Recruitment agencies can also be useful options for busy doctors who would like assistance in finding permanent jobs. With some agencies, you can just sign up and indicate that you are looking for jobs in certain specialties and certain areas and wait until they have identified one for you.
Now in most cases, if you have the time to look for yourself you can probably identify these vacancies. But an agency might cut down that work for you and also help you to get your application in early and serve you up to the employer as what is called a “hot prospect”. That’s a candidate that potentially has other offers. Which normally motivates the employer to want to speak to you.
Sometimes medical recruitment agencies are directly employed by hospitals and health services to identify candidates. This is commonly referred to as “headhunting.” In this case, it is unlikely that the position is being widely advertised or possibly that it has been advertised previously.
This approach is generally used in one of two cases and mostly for senior medical practitioner posts.
Firstly, the hospital or service may have a critical doctor leadership position that they are trying to fill and want to spend some extra money to ensure that they can find a great candidate or hopefully more than one great candidate.
Secondly, the hospital or service may have critical long-term vacancies that they have struggled to fill in the normal ways.
In both these circumstances, the agency is really your only route to applying for the job.
But you do not necessarily need to be registered for the vacancy. Often times the agency will seek you out. Most often via social media profiles. This is another good reason to start a LinkedIn profile by the way.
Using Medical Recruitment Agencies To Relocate
If you are from another country and looking to secure a position in Australia. And you are in a preferred category. Then going with a medical recruitment company may make a lot of sense. It is quite possible to gain a specialty position in Australia as a SIMG and often time the hospitals or health services will provide a lot of assistance. But a medical recruitment company can also make the process a bit easier for you by streamlining the process, handling some of the paperwork for you, and, of course, negotiating on your behalf.
The same can go if you are just moving between places in Australia. Although I haven’t seen a lot of specialists who are already registered and working in Australia using medical recruitment agencies to move States, particularly since we brought in a national medical registration system.
How To Pick A Good Medical Recruitment Agency
I’d be interested in getting feedback from other readers in the comment sections below about how they have gone about picking medical recruitment agencies.
There is no formal specific regulation of commercial recruitment agencies in Australia. Although they are subject to certain general laws, such as the Fair Trading Act 1987 in NSW. Some State bodies do require that agencies undertake additional certification before they are able to work with public employers.
Medical Recruitment Agencies can apply to be members of peak professional groups such as the Recruitment & Consulting Services Association (RCSA) or the Australian Association of Medical Recruitment Agents (AAMRA). The RCSA has a code of professional practice and offers certification. So you can look for these to ensure that the agency is adhering to industry standards and practices.
It does of course partly depend on what reason you are looking to sign up to a medical recruitment agency. Some agencies tend to specialise more in permanent work and others in locum work. Some specialise in recruiting in certain areas of medicine.
Most agencies will at least partially list what sort of jobs they have going on their website without requiring you to register and this will give you a better guide as to what areas they work in. The number of job listings also gives you a bit of an indication as to how well established they may be and how successful they are.
However, you should not necessarily disregard up-and-coming recruitment agencies. These are generally formed when a good recruiter decides to leave one of the big agencies and strike it out on his or her own. Sometimes this means you get personalised service, Jerry MaGuire style.
Probably the best way to decide on a company is to ask around any colleagues who have worked with one in the past and get their recommendations. I’d recommend signing up to more than one initially so that you can compare the overall quality of the service.
A List of Some of the Major Medical Recruitment Companies in Australia
Medical recruitment agencies generally work on a commission which they generally take from the employer. So if they don’t place a doctor they do not get paid. Commissions can vary widely but can be as high as 20% in some cases. As a doctor, it is important to understand that this commission does not come from your package it is calculated on top of your package. So if you are on a permanent placement you should get the same rates of pay as your peers. And if you are on a short-term locum placement you are obviously getting premium rates of pay anyway.
Do I need to be signed up to a medical recruitment company to do a locum?
No. But it often helps. I have myself arranged to do some locums directly with services and it is possible and the service likes not having to pay the additional premium. But if you are thinking of doing locums regularly then an agent is probably the better way to go.
Do I need to sign up to just one agent or can I sign with more?
If you are working as a locum you are not obliged to sign with one company. In fact, it probably makes sense to sign with more than one initially. As no one company has access to all the jobs that may be available. You also may find that by working with a range of agencies you find one or two that suit your needs better. Many doctors who work for a while will settle with one particular agency as their preferred agent.
Can I Work Locums As An International Medical Graduate?
It is essentially impossible to work as a locum as an IMG because of the requirement to be supervised in your initial registration period. Certainly, after you have obtained general or specialist registration you may then be able to do locums. But you may still be limited because of visa requirements.
What happens to my continuing professional development when I work as a locum?
If you are locumming as a specialist then you should continue to perform whatever continuing professional development (CPD) requirements are expected of you in that specialty and under your college. You should also consider whether your locum work is taking you out of your normal scope of practice and whether you need to tailor your CPD program accordingly. If you are not a qualified specialist then you will need to actively consider your CPD. The Medical Board assumes that doctors working as prevocational trainees and trainees under a college program are doing sufficient CPD. But once you are not in formal training the Medical Board expects that you will put together a plan and requires a self-directed program of at least 50 hours of CPD to be completed in an annual period from 1 October to 30 September each year. The 50 hours must include a mandatory practice-based self-assessed reflective element/activity of either: a clinical audit, OR a peer review OR a performance appraisal.
This is part of a new series focusing on how those doctors involved in the candidate selection process can help improve the outcomes of selection.
Having spent decades reviewing CVs, designing jobs. And, of course, sitting across the desk from interview candidates, I have learnt a thing or two about how to select well. So what sort of things would I teach the younger me about doctor selection if I had a chance all over again? Well. One of the things I would probably start with is how to write good doctor job interview questions.
Writing a good interview question for doctor selection involves:
First, understanding the key tasks of the actual job.
Second, developing a list of Key Result Areas. Things that are critical for the doctor in the job to be able to do.
Third, Developing clear selection criteria to reflect these Key Result Areas
And only then writing interview questions to assess candidates abilities to perform these key result areas.
Added to all this its almost essential to engage “job experts” – the doctors actually performing the job right now in the job analysis and criteria development and to think about other selection tools that can also aid you.
Job analysis and design.
Job analysis and design is a critical component in achieving good outcomes in any selection process. It involves examining the job to understand what knowledge, skills, attributes and values will result in a successful outcome. Research indicates that effective job analysis can contribute about a ffifth to the successful hiring of a candidate.
Ideally every time you advertise a position you should really review it again. However, for many doctors jobs, particularly trainee doctor jobs, which recycle every year, it may not be practical to do a full job analysis each year. And, arguably things don’t change that often to require an annual review. But it is worth considering doing this regularly, perhaps every 3 years.
The process of job analysis commences with reviewing the knowledge, skills and attitudes required for the position. This process gives you insights into what the outcomes of the job are and the key result areas.
For example, a key result area for a General Surgical Trainee might be ensuring that all surgical referrals for the team that come from the emergency department are seen and reviewed in a timely manner. This information then enables the development of selection criteria which will be the mechanism by which determinations are made about applicants’ suitability for the job as well as what the best tools, including interview questions, maybe for making such selections.
What’s The Hardest Bit of The Job?
Its often good to think about what the hardest part of the job maybe. The thing that new incumbents find challenging or the thing that can make the difference between a good performer and a not so good performer. This can often form the basis of more rigorous assessment of candidates, including reviewing their CV, referee checks, other assessments and of course the interview questions. Depending on how much time you have to interview you might even wish to allocate a fair part of the interview time to assessing this key result area, including using atypical means, such as a skills test or getting the candidate to give a presentation.
As an example, it might be decided that the hardest part of the job for a new psychiatry trainee might be being able to present a patient for an order to the mental health inquiry.
In which case, the selection panel might decide to ask candidates to come for the interview 30 minutes earlier. Candidates are then given access to a set of notes and a short video with a simulated patient and given the task of preparing how they would report to the inquiry. As the first part of the interview candidates are asked to outline the reasons why the patient requires further detaining in hospital.
There’s A Big Difference Between Competence and Performance.
Competence is what a doctor can do based what they have been trained to do so far. We can often assess this from what they say in their CV and to some extent their referee reports.
Performance is what a doctor actually does day to day.
Performance depends on competence however, it is also influenced by a host of other factors.
Obviously, a level of competence is required for any doctor job. But it is the performance that counts at the end of the day. Unfortunately, performance is often harder to assess than competence as it often calls for real-world situations.
Capability Frameworks Can Sometimes Be Useful If You Don’t Have The Time.
Many health departments have developed capability frameworks which describe the broad competencies and performance for staff. They describe the types of knowledge, skills and attributes required. Often times some of the language from these frameworks automatically populates into job descriptions within the e-recruitment system.
Every Specialty Medical College in Australia and New Zealand has defined a framework for its Fellows and Trainees. Most are based on the internationally recognized CanMEDS Framework. These can be quite useful reference documents when developing job descriptions as they tend to cover the range of capabilities that doctors need (e.g. communication, teamwork, medical expertise, leadership skills, patient advocacy etc…) And if used well you can use these frameworks to develop selection criteria which reflect where a doctor should be developmentally against these frameworks.
So for example a job description for a Resident Medical Officer might indicate that their management skills should reflect knowledge of key management tools and demonstration of effective time management. Whereas a job description for a Consultant might reflect that their management skills should demonstrate respect for the role of managers and active participation in unit leadership and management tasks, including people development and conflict resolution.
Can job analysis & design incorporate competency-based frameworks in medical trainee recruitment?
UK authors Plint and Patterson have demonstrated that we can predict progress in doctor training and job performance by conducting a thorough job analysis. In their 2010 study the authors conducted job analyses to develop selection criteria for general practice training. They then designed selection instruments and methods to evaluate candidate’s capabilities against these criteria and using a validation process to assess the extent to which selection methods provide valid predictors of progress in training or job performance.
However, one general distinction between competency frameworks and selection criteria is that competency frameworks often call for much greater numbers of criteria than which may be allowed for an individual job.
So the task if using a competency framework is to distil all this information into key criteria. Again, nothing beats a proper job analysis for this.
Enter The Job Expert.
All of this work can be made infinitesimally easier if we engage the actual job experts. Who are the job experts I hear you say? They are the people successfully doing the job right now. Which in Medicine, for example, means most of us.
I am amazed how often for trainee doctor interviews the panel is comprised of people who have either never done the actually trainee job, not worked closely with trainees or have been a trainee once 2 or more decades ago.
Having such a panel for trainee selection is just giving yourself an automatic handicap from the outset.
Job Experts on selection panels is considered best practice in many industries. But not medicine it seems.
Incorporating at least one doctor on the panel who is currently in the role can save you time in developing the right selection criteria, the right selection approach, the right questions and they generally also have a gut feel for which candidates will not be good fits.
So why is there such resistance to including trainee doctors on trainee selection panels?
Reasons For Resistance.
Possibly the main reason for resistance is tradition and a lack of understanding of the additional value a job expert brings to the table in selection.
Another problem can be that often trainee selection panels are hotly contested with lots of stakeholders (hospitals, training directors, colleges) wanting to ensure that their input is considered. So often the trainee on the panel can be jettisoned if there are already too many players.
Finally, it may be difficult for trainee themselves to participate in selection. They may feel that they are judging their peers or that they have not yet “earned the right.”
So What About Doctor Job Interview Questions?
Most recruitment manuals or training programs will suggest that interview questions should fristly be developed based on the selection criteria and then wherever possible put in a behaviourally-oriented way as a Past Behaviour Question (PBQ).
PBQs are questions which ask for examples of past behaviour. They tend to be recommended by HR exerts over “situational questions” (SQs), i.e. questions which ask an applicant what they would do in a particular situation.
The reason that PBQs are recommended is based on the idea that past behaviour is a better predictor of future performance. And there is some research that has demonstrated that PBQs may be more discriminative than SQs and that candidates find it harder to manage impressions (fake responses) in PBQs.
The aim of PBQs is for
the applicant to demonstrate through past behaviour that they are able to
demonstrate the selection criteria.
When asking about behaviours,
interviewers can note applicant responses according to the CAR approach:
Context: what the situation was.
Action: what the candidate actually did (as opposed to what others did).
Result: what the outcome(s) of the candidate’s action(s) were.
Lets take an example of such an approach to developing an interview question.
Lets say that it is determined that one of the essential criteria for an Anaesthetic Training post is that
The trainee demonstrates the ability to practice in a safe manner in the operating theatre and recovery.
A behaviourally oriented question could then be developed around this question, as such
“Please describe a time when you identified a safety issue in the operating theatre or recovery, or another similar setting. What was the situation (context), what was your involvement (action) and what were the outcomes (result)?”
A Problem With The Behaviour Approch?
The problem with PBQs is that many doctors are accustomed to answering PBQs and have little difficulty providing answers. Strong candidates may even suggest examples to questions which are not put in a behavioural format. It is not absolutely certain how to discriminate between a candidate who has clearly done their research and practiced answering in such a format versus one that has not. My preference would be to reward the cadidate that bothered to prepare.
On the other hand, it is also not uncommon for some candidates to miss or avoid the requirement to provide an example. Such doctors may attempt to answer in a hypothetical way. If this occurs the person asking the question should redirect the candidate to providing an example. If the candidate is unable to provide a suitable example, then it is best to complete the question and move on to the next and rate accordingly.
The CAR approach is sometimes referred to as the STAR approach
(Situation, Task, Action, Result), in which case questions are often asked
along the lines of: “Describe the situation that you were in or the task you
needed to accomplish.”
Is there a Role for Situational Questions or Clinical Problems in Interview?
In short Yes. whilst, the PBQ has come to be considered the gold standard approach to selection interviewing based particularly upon evidence accumulated from a range of studies in the 1980s and 1990s. However, recently Levashina et al (2014) re-examined some of the commonly held beliefs in relation to selection interviewing. This research indicates that the difference between SQs and PBQs may not be as dramatic as previously thought.
Selection studies have demonstrated that both PBQs and SQs in traditional panel interviews have comparable reliability and acceptability. But PBQs possibly have less “fakeability” and higher predictive validity for high-complexity jobs than SQs.
In particular, a mix of SQs and PBQs within a doctor interview format may be a valid approach and an area worthy of more study. Yoshimura et al (2015) in a study of 26 medical graduates applying for specialty training reported both PBQs and SQs as equally reliable and acceptable in a multiple mini interview format.
One popular use of SQs in doctor interviews is in the format of a clinical problem in the interview. I understand why panels feel the need to introduce a clinical problem to the interview. After all, the doctor will be doing clinical work. But there are quite a few problems with this approach.
The clinical problem will inevitably only test a small amount of knowledge and understanding of whatever field of medicine we are interviewing for. So how do we account for the false positives (the candidates who got lucky and were asked a question in one of the few areas they were good in) versus the false negatives (the ones who got unlucky and hadn’t brushed up on that particular topic)?
There are actually better ways of assessing clinical knowledge. Such as actual tests of clinical knowledge.
Practically these questions tend to take up a lot of time in the interview. Especially if the candidate has to read through a complex scenario and ask clarifying questions.
Where I am okay with a clinical problem being asked is where it may be being used to set the context for assessing broader competency issues, such as a doctors approach to collaborating with others or practicing safely.
But again if being able to successfully deal with a certain type of clinical situation is deemed essential for the role perhaps its better to ask the doctor candidate themselves for an example.
Related Questions.
Question: What sort of other selection tools are helpful in improving selection in doctors?
Answer. A number of innovations have been made in the space of doctor recruitment lately. As mentioned in this article when there is a situation of large or mass candidate selection. For example selection into a basic training program. Then a number of additional selection techniques can be applied.
You can test candidates before the interview. A couple of common tests are clinical knowledge tests and what are called situation judgement tests. These can be used to screen candidates to reduce the number interviewed overall and/or included in the final overall assessment.
You can interview candidates more often. The most common way this is done is called the MMI or Multiple Mini Interview. This is often done for medical school applications. Instead of being interviewed by one panel candidates progress around a series of rooms with one or two assessors in each who quiz them on specific areas of selection.
Even in smaller interview batches you can include more value in your selection by:
including a skills test where appropriate (i.e. getting the candidate to demonstrate a key skill for the role, for example tieing a surgical knot)
collecting references before the interview and asking the referees the same questions that you will be asking the candidates
Question: Is there a good all round doctor interview question?
Answer. The problem with all purpose questions can be that candidates have prepared for them. It would be easy to say that you should always tailor your questions to the role. However, questions like:
“How does your experience and skill set make you a good candidate for the role?”
As somebody who has reviewed 1000s of applications from international medical graduates for oftentimes scarce roles in Australia, I have had the opportunity to correlate English testing score performances with job candidate performance as well as real-world performance in the job. I’ve also spoken with many other doctors who do job selection. I’d like to share some insights with you about the English proficiency standards and English Requirements for doctors working in Australia. What I intend to share with you is the knowledge you ought to have but which is actually not normally shared with candidates.
But first of all. It is not surprising that the focus of many international doctors in seeking employment in Australia is working out what the required medical board standard for English proficiency is and how to meet this. On this blog, I often write that answers to questions in medical recruitment are sometimes complex.
But actually the answer to the question of what English Test score do I need to satisfy the Medical Board of Australia requirements for registration is reasonably straightforward. The Medical Board of Australia will accept the following language tests and results for international medical graduates (IMGs):
IELTS Academic module. The IELTS score for doctors in Australia is a minimum overall score of 7 and a minimum score of 7 in each of the four components (listening, reading, writing and speaking).
OET with a minimum score of B in each of the four components (listening, reading, writing and speaking
PTE Academic with a minimum overall score of 65 and a minimum score of 65 in each of the four communicative skills (listening, reading, writing and speaking)
TOEFL iBT with a minimum total score of 94 and the following minimum score in each section of the test: 24 for listening, 24 for reading, 27 for writing, and 23 for speaking.
Perhaps It Is a Little Bit More Complicated Than That.
OK, it is actually a little bit more complicated than this because the Medical Board will also accept successful completion of the following tests as evidence of English language competency:
the New Zealand Registration Examination (NZREX) administered by the New Zealand Medical Council
the PLAB test administered by the Professional and Linguistic Assessments Board of the General Medical Council.
Aggregation of Results
And in addition, for each of the above-mentioned tests, the International English Language Test (IELTS), The Occupational English Test (OET), The Pearson Test of English Academic (PTE Academic) and The Test Of English as a Foreign Language Internet-Based Test (TOEFL iBT), the Medical Board of Australia will now accept an aggregation of results across two separate tests.
So for example, for the IELTS score for doctors in Australia, you can aggregate your scores across two tests such that you can count scores from either test to come up with 7 or more across the 4 domains. As long as you do not score less than 6.5 on any domain in either test. So if you get a 6.5 in listening on one sitting you can fix this by getting a 7 on a future test.
The Minimum Standard Is Not Going To Get You Very Far
Whilst the focus on achieving the minimum standard is understandable its actually a distraction from what international doctors ought to be focusing on, which is being able to demonstrate effective communication skills.
You see in order to be registered as a health practitioner in Australia, the Medical Board and the Australian Health Practitioner Regulatory Authority say that you “must be able to demonstrate that your English language skills will enable you to safely practice your profession.”
Safe To Practice Or Good Practice?
But this only part of the point. There is also the issue of being able to effectively practice your profession or even practice your profession at a high standard.
So why is it that the minimum score may not be sufficient for you. Well actually there are a couple of main reasons and I will take you through each of them in turn.
Your English Proficiency Score Is An Indicator Of Your Ability to Communicate
At the end of the day, you always want to pass the test. But if you are studying to pass an English language test you really should be asking yourself the question. “How good is my English and how good do I need it to be?”
If you are studying to pass an English language test you really should be asking yourself the question. “How good is my English and how good do I need it to be?”
Dr Anthony Llewellyn
To illustrate my point lets look at the most common test that International Doctors take the IELTS score for doctors in Australia. Let’s consider what IELTS itself says about the scores that you may receive on their test.
The IELTS test delivers a result of 0 to 9 in each band, as well as overall. Regardless of which testing component you score the meaning assigned to each band is as follows:
Meaning of IELTS score for doctors in Australia
Band
Meaning
0
The test taker did not answer the questions.
1
Non-user. The test taker has no ability to use the language except a few isolated words.
2
Intermittent User. The test taker has great difficulty understanding spoken and written English.
3
Extremely Limited User. The test taker conveys and understands only general meaning in very familiar situations. There are frequent breakdowns in communication.
4
Limited User. The test taker’s basic competence is limited to familiar situations. They frequently show problems in understanding and expression. They are not able to use complex language.
5
Modest User. The test taker has a partial command of the language and copes with overall meaning in most situations, although they are likely to make many mistakes. They should be able to handle basic communication in their own field.
6
Competent User. The test taker has an effective command of the language despite some inaccuracies, inappropriate usage and misunderstandings. They can use and understand fairly complex language, particularly in familiar situations.
7
Good User. The test taker has operational command of the language, though with occasional inaccuracies, inappropriate usage and misunderstandings in some situations. They generally handle complex language well and understand detailed reasoning.
8
Very Good User. The test taker has fully operational command of the language with only occasional unsystematic inaccuracies and inappropriate usage. They may misunderstand some things in unfamiliar situations. They handle complex and detailed argumentation well.
9
Expert User. The test taker has fully operational command of the language. Their use of English is appropriate, accurate and fluent, and shows complete understanding.
Do You Just Want To Be a Good User?
Let’s think about the implication of being deemed to be at Band 7. A “Good User”. Being a “good user” means that you occasionally deliver inaccurate information. Or occasionally use the wrong word. Or occasionally misunderstand in some situations. You will generally (but not always) handle complex language and detailed reasoning.
Working effectively in medicine in Australia is all about communication. You really cannot afford to be occasionally misunderstanding a patient as this might lead to a serious outcome, such as an error or a conflict. Given the amount of communication that goes on in a hospital and the level of complexity of communication and language your “occasional” problems are likely going to translate into being at least once a day if not more often.
Employers Evaluate Your English Proficiency Score Differently to AHPRA
Employers know that there is a big difference between a straight-set of 7s on an IELTS or a set of Bs on an OET versus having at least one 8 or an A. The higher your overall score the better. Selection panels definitely do take this into consideration.
Selection panels do it when they review the initial applications in what is called the “culling phase”. So a classic example might be a situation where for example there are 20 IMG applicants for one job and only 6 interview slots. If the candidates are equal in all other ways then those with just the minimum scores for English language requirement may well be placed in the “non-interview” pile.
Even when interviewing candidates selection panels will be more keen to see the candidate who has a good result on their test. And will more intensely scrutinize candidates with lower scores to see if there are any significant communication concerns.
So my best advice for any doctor who does, unfortunately, need to prove their English proficiency is to study and work on your English with the end aim being that your English communication should not get in the way of you being a good doctor in Australia.
Related Questions
Question: How long does an English Language Test last for?
Answer: Generally the Medical Board will accept a test that is less than two years old. So this often means that applicants are re-sitting tests as you may sit an English test for one particular purpose, such as to do a course and by the time it comes around to applying for registration for a job your test is out of date.
Question: Do I need an English Language Test to sit the Australian Medical Council exams?
Answer: Surprisingly the answer to this question is no. Of course, both the written and clinical exams are done in English so if your English is poor you are going to struggle with them. It’s probably sensible to wait till after you pass your MCQ to sit an English test if you need to do it. This hopefully avoids the issue of the test result expiring before you are offered a position.
Question: Do I need to do an English Language Test if I have studied in English?
Answer: This is actually a very complex question to answer. Even some Australian doctors who have done high school in Australia, as well as medical school in Australia, can end up having to do an English test if they are unable to provide evidence of their high schooling for example. Even brief stints studying or working overseas can create a problem.
Other than doing an English language test there are 3 alternate pathways (the Board loves pathways) to proving your English language proficiency with the Medical Board. These are:
Primary language pathway
Combined secondary and tertiary education pathway, and
Extended education pathway
As an example. Even if English was not your primary language. If you can prove that you have studied continuously in English in higher education for 6 years you satisfy the requirements under the Extended education pathway. For a more detailed explanation of your options, you can hop over to the relevant FAQ page on the Medical Board website.
Question: Do I need to keep doing English language tests when I am registered?
Answer: Generally no. Once you are registered in Australia it is assumed that you are working in English and therefore maintaining your skills. If you have a large break in employment or registration or go overseas for a significant period to work, however, you may need to check with the Medical Board again.
This Post is Part of a Series on All You need to know about the Medical Career Pathway in Australia.
If you search enough on Google and look enough on facebook you will readily find lots of opinions about the Australian Medical Council examinations process. Given that a lot of the readers of this blog are international doctors we wanted to present you with some factual information about the AMC exams. So we have engaged some real doctors who are currently going through or have been through the process.
In relation to the question about how hard the Australian Medical Council Exam is. The answer to this obviously depends on a range of factors, including how much time you put into preparing for the exam and how close your own medical school training is to the Australian context. There are actually two separate exams to complete the AMC. A Part 1 Multiple Choice Exam and a Part 2 Clinical Exam. According to the latest report from the AMC in one year, there were 2663 AMC MCQ (Part 1 Exams) sat with 1,559 candidates passing. That’s a pass rate of about 58%. For the AMC Clinical Exam 597 candidates passed out of 2,165 candidates assessed. That’s less than a 28% pass rate. So we would say that the first part of the AMC exam is fairly hard and the second part is extremely hard.
Read on to find out more about the process of the AMC Exam, including how best to prepare.
Eligibility Requirements for the Australian Medical Council Exam
In order to be able to sit for the AMC Exams you must first establish what is called a portfolio
You first create a registration with the AMC website.
You should also check that your medical degree is awarded by an institution recognized by the AMC. The AMC recognizes most but not all medical schools which are listed with the World Directory of Medical Schools. There is a handy search on the AMC site.
You must then also create an EPIC account and confirm your identity with the ECFMG (located in the United States).
You get an EPIC id in about 3 working days, which you use to establish your AMC portfolio.
You upload your qualifications to EPIC. As you do so YOU MUST REQUEST that EPIC send a report to the AMC.
EPIC notifies you and the AMC when they have completed their check.
This whole process will cost you $500 AUD to register with the AMC and about $205 USD for EPIC (more if you are wanting more than one qualification verified).
Once EPIC reports back in the affirmative to the AMC you will be allowed to request to sit for the AMC Part 1 Examinations.
There is no actual work experience requirement to sit the AMC Part 1 Examination and you can, in fact, start preparing for this whenever you like. But of course, you will not be able to sit the exam without a verified medical degree. So you can start studying for it in medical school but won’t be able to sit it till after you graduate.
The Part 1 MCQ Examination
The AMC Computer Adaptive Test (CAT) MCQ Examination is a computer-administered fully integrated multi-choice question examination delivered in one sitting that lasts 3 and a half hours.
There are regular invigilated examinations in Australia as well as a number of sessions available in examination across the world.
The examination itself consists of 150 “A-type MCQs”. You must select the one correct response from amongst five options. 120 of the questions are “live” questions, which mean they count towards your score. The remaining 30 questions are being piloted and don’t count towards your final score. You do not know which questions are being piloted so you have to give your best for all 150.
You are expected to complete all 150 items and must complete the 120 scored items. Failure to complete all 120 scored items in the examination may lead to insufficient information for a reliable determination of your ability and therefore a result on the AMC adaptive scale.
According to the AMC the MCQ Examination
focuses on basic and applied medical knowledge across a wide range of topics and disciplines, involving understanding of the disease process, clinical examination, diagnosis, investigation, therapy and management, as well as on the candidate’s ability to exercise discrimination, judgment and reasoning in distinguishing between the correct diagnosis and plausible alternatives.
AMC MCQ Examination Booklet
So the questions are a mix of more basic knowledge as well as clinically focused. The standard is set at the level of a newly qualified graduate of Australian medical schools, who is about to commence intern training.
The content is “blueprinted” according to patient groups as follows:
Adult Health (Medicine)
Adult Health (Surgery)
Women’s Health (Obs) (Gyn)
Child Health
Mental Health
Population Health
TOTAL
35
25
15
15
15
15
120
There are many different books you can study to pass the exam but there is no right or wrong answer to which book needs to be studied. The AMC has a long list of books and other sources that they recommend for the examination some of which can only be bought in the AMC bookstore.
You may read all the books in this world and still fail or you may read just one book and pass the exam. Many candidates are currently preferring to study John Murtagh’s General Practice book. Along with this it is important to be practising examination questions. So you really should study the Handbook of Multiple Choice Questions with explanations and try to do as many past papers as possible.
Some candidates still prefer to do Kaplan USMLE Step 2 lecture notes in place of John Murtagh. The advantage of Murtagh over Kaplan notes is that Murtagh can be studied for the clinical exam also.
You should practice as many MCQs as you can. There is also an official online practice exam through the AMC website.
Strict Rules For the MCQ Examination
Sitting the AMC Exam involves first registering to do the exam with the AMC and then paying the required fee. You then must register with the exam centre vendor which is currently Pearson-Vue. You have a 12-month authorisation period to select an exam. You can change your exam venue within a limited period of time but once you are locked in it is difficult to alter your date and time.
You need to bring appropriate identification with you on the day.
There are strict rules for the MCQ exam which you must abide by. You should read all the official instructions carefully. You are not allowed to bring tissues (e.g. Kleenex), paper of any kind, pens/pencils, or rulers. Your mobile phone must be switched off and placed in an allocated area of the room. Bags are also placed in the allocated area of the room. Food and drinks are not allowed in the computer examination room.
They provide you with a whiteboard and pen for making notes. The whiteboard is collected by examination supervisors at the completion of the examination.
Family members are not allowed to wait in the examination venue. They must wait outside the building of the examination venue.
Because the MCQ exam is computerized you will receive your result fairly quickly in about 4 weeks. You get a print out which indicates where you performed overall, as well as the range for all candidates appearing for that particular exam. You also get a breakdown of your performance in the question domains. This is useful if you don’t pass to know where to put your efforts next time.
You need to score 250 or more to pass. Less than 60% of candidates pass. Although this score is probably depressed somewhat by those candidates sitting more than once.
It currently costs $2,720 to sit for the MCQ.
The AMC Clinical Examination Part 2
Once you pass AMC MCQ exam, you are then able to appear for the AMC Clinical exam. These are all held in Melbourne at the AMC’s purpose built examination centre.
Clinical Exam Format
The Clinical exam format is a 20-station multidisciplinary structured clinical exam which assesses your skills in Medicine, Surgery, Gynecology and Obstetrics, Pediatrics, and Psychiatry. There are 14 scored stations, 2 pilot (non-scored) stations and 4 rest (non-scored) stations.
As of 2019 the result is graded as either clear pass or clear fail. Prior to this borderline candidates were offered a retest. However, the AMC found that the time between examination and retest was becoming so long that the results were not meaningful.
You must pass 10 or more of the stations to pass the exam. The pass rate is incredibly low. About 28%
It is recommended that you should study the Handbook of Clinical Assessment and practice roleplays as much as you can. You may want to attend a course. Candidates also study different notes such as Karen notes, and the VMPF notes. John Murtagh’s General Practice is also worth revising.
It is extremely wise to form a study group and there are many groups around where you can practice what is called “recalls”, which is when a candidate who has previously sat the exam attempts to reconstruct the station.
The cost of sitting the Clinical Examination is currently $3,530.
Frequently Asked Questions
Question: What If the AMC does not recognize my medical school?
Answer: It is possible that your school is new or has not been considered by the AMC. Check first that it is on the World Directory of Medical Schools. You can enquire of the AMC if they will accept your school but there is no guarantee.
Question: How often can I sit the MCQ exam?
Answer: As many times as you want. But given its cost, most people try to only sit it once. Like most other exams your chances of passing are best the first time and diminish over time.
Question: How often can I sit the Clinical exam?
Answer: You can sit as many times as you want but there has often been a backlog so the AMC over the years has tended to prioritize newer candidates. Again it costs a lot of money to sit this exam and your chances of passing diminish as you repeat the exercise.
Question: Do you need to clear one of the English language tests, such as IELTS or OET to sit for the AMC MCQ Part 1?
Answer: No. It might be wise to put this off till after you have passed the MCQ Part 1 as there is a time limit over which the result can be accepted.
Question: Do you need to have cleared the English language requirements, such as evidence of comparability or the IELTS or OET to apply for an internship and a work visa?
Answer: Yes, you definitely do. Unless you can prove your English language proficiency in other ways, which is normally difficult for most IMGs.
Question: How high should you score in your English test?
Answer: From a regulatory point of view an overall band score of 7.0. with a minimum of 7.0 in each component is required for the IELTS. Similarly, for the OET, an overall score of B and a minimum of score B in all four components is required. However, many employers will look at these results and look for candidates with even better scores than the minimum.
Question: Do you need to clear the AMC Clinical Exam Part 2 to apply for a position?
Answer: No you don’t. But if you get a position prior to completing your Part 2, you will have to clear it as part of your provisional registration before you can apply for general registration. Generally speaking candidates with both AMC Part 1 and 2 are preferred by employers. over just Part 1.
Question: Are their alternatives to the AMC Exam process?
Answer: For an IMG coming through the Standard Pathway there is no alternative to sitting the MCQ.
If you don’t wish to come through the Standard Pathway then your only other options are to try to gain full registration in one of the other competent authority pathway countries first, for e.g. completed the PLAB in the UK. But if your ultimate goal is to work in Australia then this is really delaying things.
In relation to the clinical examinations, you may be eligible to undertake a workplace-based assessment as an alternative to the AMC Clinical Examination if you are able to gain a position at one of the 10 services which are authorised by the AMC to conduct a workplace-based assessment for the AMC Certificate.
Services which offer Workplace Based Assessment
Program provider
Location
Central Coast Local Health District
Gosford and Wyong, New South Wales
Flinders Rural Health SA
Mount Gambier Hospital, South Australia
Hunter New England Local Health District
Newcastle, Armidale and Tamworth, New South Wales
Illawarra Shoalhaven Local Health District
ISLHD Hospitals, New South Wales
Launceston General Hospital
Launceston General Hospital; North West Regional Hospital, Burnie; and Royal Hobart Hospital, Tasmania
Mid North Coast Local Health District
Kempsey District Hospital (with some support from Port Macquarie Base Hospital), New South Wales
Monash Health
Victoria
Rural and Outer Metropolitan United Alliance (ROMUA)
Goulburn Valley Health, Shepparton, Victoria
WA Country Health Service
Bunbury, Geraldton and Kalgoorlie, Western Australia
Whilst the number of enquiries for help I have had from US doctors is slightly less than say, for example, UK doctors, the prospects for US doctors working in Australia are pretty much on a par. There are a couple of main options for US doctors to work in Australia.
So the answer to the question can US doctors work in Australia is yes. Of course, no doctor coming from another country is guaranteed to be able to work in Australia. But because the US medical training system is recognised by the Medical Board of Australia as being on a par with that of Australia, US doctors tend to have good success with either becoming generally registered through what is called the competent authority pathway or being recognised as a specialist through what is called the specialist pathway. In 2017 (the latest year we have figures for) 20 out of 23 US specialists were deemed comparable to work in Australia.
So the prospects for working in Australia as a US doctors are good. But its important to give a little bit more detail. As I have highlighted there are two main options for getting registered so we will talk about these first and then go into some other common questions.
The Competent Authority Pathway. The Trainee Option For US Doctors Australia.
If you are a trainee doctor in the US, i.e. a Resident who has not yet achieved specialty status. Then you are looking at the competent authority pathway for working in Australia.
The competent authority pathway assigns preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States and the Republic of Ireland.
The rationale for this is largely an historical one and based on the premise that all these jurisdictions have similar approaches to medical school training and similar standards.
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools, the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically as those from Australia.
If you are an international medical graduate and you have achieved general registration in the United States, Canada or the United Kingdom (but not the Republic of Ireland) you are also eligible for the competent authority pathway.
What are the steps involved for the competent authority pathway.
Applying to the Australian Medical Council for primary source verification
Applying for registration to the Medical Board of Australia
Completing 12 months supervised practice
Applying again to the Medical Board of Australia for general registration.
Eligibility for Competent Authority
You can do a “self-assessment of your eligibility for the competent authority pathway on the Medical Board of Australia website here.
The essential requirements are:
Successful completion of the United States Medical Licensing Examination Step 1, Step 2 and Step 3 since 1992
AND
Successful completion of a minimum of two years of graduate medical education within a residency program accredited by the Accreditation Council of Graduate Medical Education.
OR
Successful completion of the National Board of Medical Examiners (NBME) licensing examinations Part I, II and III before 1992
AND
Successful completion of a minimum of two years of graduate medical education within a residency program accredited by the Accreditation Council of Graduate Medical Education.
This means doctors who have trained in US accredited medical schools outside of the United States sometimes find it difficult to come to Australia via the Competent Authority Pathway.
See if you qualify for a free coaching call to explore your options working in Australia
[fluentform id=”8″]
What types of jobs can I apply for as a US Trainee?
You can pretty much apply for any sort of trainee job. There are often a number of postgraduate years 2 or 3 general jobs on offer, which are generally termed Resident Medical Officer in most States and Territories but may also be called House Officer or Hospital Medical Officer in some places.
Above these posts normally come the specialty training positions (Australia is a bit different from the US in that there is a period between medical school and specialty training) which are generally referred to as Registrar positions. But you might also see advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most of these jobs will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice (which is what we call family medicine in Australia), the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
your previous experience, especially in the type of position for which you have applied
whether you have practiced recently and the scope of your recent practice
the requirements of the position including the type of skills required for the position
the position itself, including the level of risk, the location of the hospital or practice and the availability of supports (supervisors)
the seniority of the position, for hospital position
In general you will either be approved for Level 1 or Level 2 Supervision. There are 4 Levels and the higher up you go the less direct oversight you require.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times and you must consult with them about all patients. Remote supervision (for e.g. by telephone) is not permitted. Level 1 is generally recommended when you are very junior yourself or entering a junior role which you are not very familiar with. In Australian major public hospitals there are many layers of other doctors who you can get supervision from so Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision, which is what most US trainees approved to work in Australia will normally be approved for is a step up from Level 1 Supervision. Supervision must primarily be in person but your supervisor can leave you to do work on your own and you can discuss by phone. You should discuss with them on a regular (daily) basis what you have been doing with patients. But do not need to discuss every case.
What happens after I commence my position?
Once you are approved for registration and you have your visa issues sorted you will be able to commence work. Generally your employer helps you out with all these things. You will be working under what is called “provisional registration” by the Medical Board of Australia. Generally all you need to do for this 12 months is to pay attention, show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia and it is your responsibility, not theirs to see that they are completed and returned on time. If all the reports go well you will be able to be recommended at the end of the 12 months for general registration.
You will probably be starting to look for another job or negotiating an extension around this time. With general registration you may be able to apply for a skilled visa, as well as be looking at applying for permanent residency.
Permanent residency is crucial for applying for most specialty training programs. See below.
The Specialist Pathway. The Option For Specialists US Doctors Australia.
For US specialists your option for working in Australia is what is called the Specialist Pathway.
Once again this starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need Position, in which case the employer or recruitment agent will provide you a lot of support and will likely pick up the costs of being assessed.
For most International Doctor specialists however these days you will be approaching the college directly to be assessed. This is not something to be trifled with. The paperwork requirements and the cost (generally around $5,000 AUD and more) is considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
I have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The other issue for US specialists is that there are more than 2x the number of specialties in the US than in Australia. So working out which specialty goes into which Australian college can also be confusing. Fortunately, I have you covered on that as well here.
After you go through your specialist assessment you are given an outcome. In the majority of cases for US specialists, you are deemed either partially comparable or substantially comparable. Rarely are you deemed not to be comparable by the college. If you are this means you cannot directly become a specialist in Australia. You will have to go through the competent authority route and re-enter training.
Can you enter training in Australia if you are a US doctor?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in most also at least permanent residency.
There is an alternative but time limited pathway for US doctors who are just seeking a short term experience in Australia to add to their training in the US. This is called the Short Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed you training in the US or be less than two years from completion. So this is a program mainly for early career specialists or advanced trainees.
You go through the same steps with the AMC as per the competent authority pathway to gain registration. You will not, however, be able to apply for specialist assessment as part of this pathway. But if you gain general registration you may then be able to apply for another position and then apply for specialist assessment.
Can you do your internship in Australia as a US doctor?
Basically no. Internship in Australia is a provisional year that only applies to medical graduates from medical schools in Australia and New Zealand. There is a “loophole” which only applies to doctors who have not been able to complete an internship or equivalent in their own country. But the Medical Board warns that this is not a great option and is only granted in limited cases. You are far better off starting your ACGME residency program in the US and applying after 2 years or more.
How many US doctors are working in Australia?
There no one public data source to tell us how many US doctors are currently working in Australia.
From data collected by the Australia Government we know that for 2017 (latest available year):
40 applications were made for the competent authority pathway by US doctors with 30 granted provisional registration through that pathway
29 applications were made for specialist assessment, 3 of which were deemed not comparable, 12 partially comparable and 8 substantially comparable, with a further 6 withdrawing their application
12 US doctors were recommended for specialist recognition with 4 not being recommended
Are Osteopathic Doctors recognised in Australia?
Yes. The degree Doctor of Osteopathic Medicine (DO USA) is a medical qualification that is recognised for the purposes of medical registration by many international registration authorities. The Medical Board of Australia (the Board) has agreed to accept the DO USA as a primary medical qualification for the purposes of medical registration provided that the DO USA was awarded by a medical school which has been accredited by the Commission on Osteopathic College Accreditation of the American Osteopathic Association and recognised by both the Australian Medical Council and the World Directory of Medical Schools.
How hard is it to become a specialist in Australia if you are from the US?
Specialist doctors from the United States are not automatically granted specialist recognition. As you can see from above in 2017 there were 29 applications made for specialist assessment to the Australian colleges by US doctors and of these only 20 were deemed to be comparable. In the previous year of 2016 4 applications were deemed to be not comparable, 11 partially comparable and 8 substantially comparable.
US doctors tend to get a reasonably favourable outcome in comparison to doctors from most other countries. However, many are being seen as partially comparable only which involves more work and effort to then get to the level of specialist recognition.
If we compare these results to another competent authority country, the United Kingdom then in 2017, 332 UK doctors were deemed substantially comparable, 43 partially comparable and only 5 not comparable.
Are there any particular specialties that are easier to apply for?
The majority of specialties have some vacancies and will provide opportunities for US and other IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be quite difficult.
On the other end of the spectrum general practice, psychiatry and most parts of critical care medicine are often always looking for doctors.
Are there any other options for working as a doctor in Australia?
Some doctors just want to come to Australia for a limited period of time as an opportunity to train in another country.
As we have highlighted above there is an alternative but time-limited pathway for US doctors who are just seeking a short term experience in Australia to add to their training in the US. This is called the Short Term Training in a Medical Specialty Pathway. To do this you must be offered a training position first and you must have either completed you training in the US or be less than two years from completion. So this is a program mainly for early career specialists or advanced trainees.
We hope that you found this summary about how US doctors can work in Australia useful. If you have any questions or queries or just want to relate your experience. Please feel free to leave a comment below.
A question we get asked reasonably frequently is about medical intern pay and specifically whether medical interns get paid in Australia. Often this comes from doctors working in other countries. We think the main confusion occurs around the concept of an intern in a medical setting and an intern in a corporate setting.
In relation to the question of whether medical interns get paid in Australia. The answer is an unequivocal yes. Medical Interns are paid a salary of between $68,000 AUD and $79,000 AUD base salary per annum for full-time work, depending on which State or Territory of Australia they are in. The majority of interns are employed on a full-time basis and they can often earn a little be more due to working shifts and overtime.
So the question then arises as to why medical interns are paid and other interns are not? As well as whether there are other situations where a doctor might be employed in a non-paid capacity. Feel free to read on further where we answer these questions and discuss the topic of medical intern pay.
Why Are Medical Interns Paid and Other Interns in the Corporate Sector Normally Not paid?
According to the online etymology dictionary, the word intern comes from the French word “interner“, meaning send to the interior or confine, which itself derives from the Latin word “internus“, meaning within or internal.
the French word “interne” means ‘assistant doctor’ and the word means one working under supervision as part of professional training”
So it seems that the concept of the medical intern or doctor intern came first. This, in turn, stems from the concept of an apprenticeship, which arose in the middle ages under the guild system. Agricultural methods and technology had become more advanced, requiring fewer workers in the fields. So people started leaving the farm to take up trades in their early to mid-teens.
Apprentices would pay a guild master to teach them the trade. Apprentices typically lived with the master for a decade, if not longer, and couldn’t marry or earn wages during the apprenticeship. At the end of the apprenticeship, the apprentice became a member of the guild and a “journeyman”, which meant he could earn his own wages.
Medical Interns Were Probably Not Paid At Some Point.
Therefore it’s also likely at some point even medical interns were unpaid. The apprenticeship model in medicine evolved into the concept of a medical internship year probably sometime in the early 1900s. And intern doctors became doctors who were recent graduates of medical schools who were unlicensed but able to work under supervision strictly in hospitals.
So at some point, medical intern pay was introduced for these doctors. You generally needed to complete your intern year to be able to go out on your own and start a practice. But many doctors stayed on longer and these trainees were often housed by the hospitals. This is where the term resident comes from.
For some time now. Since the end of the second world war, at least we have had medical intern pay. This is a reasonable proposition as they have already undertaken a large degree of unpaid higher education (generally more than any other profession) to get to this point and they now contribute significantly to the operation of many hospitals.
According to Taylor Research group, corporate intern programs originated in the United States in the 1960s as both businesses and government agencies saw the merit of providing short term opportunities for prospective future employers to gain some work experience in their summer breaks. However, it has only been in the late 1990s that government and corporate internships have become common in college campuses in the United States and also only in the last couple of decades have they started to become more common in other countries.
Because these internships are generally shorter and limited in time and focused around providing current students with a work experience opportunity most internships have been offered on a voluntary basis. This is not to say that no corporate internship provides payment or other benefits. In some cases, there may be allowances for things like travel or accommodation or other expenses. And of course, the premise of an internship in the corporate sector is that one receives free on the job training.
Are there situations where you might not get paid for working as a doctor in Australia?
There should really be no situation where a doctor performs work in Australia and is not paid for this. Certainly, all true medical internship positions are paid under an Award based system. Which is a set of rules that are commonly applied to a group of employees across a certain industry sector and by which the employer must abide.
Sometimes the concept of a clinical placement or clinical observership can be confused with a medical internship. These are actually quite different things.
A clinical placement in medicine in Australia normally occurs as part of the formal requirement for workplace-based experience in a medical school program. Students are assigned to placements under supervision in hospitals, general practices, and other settings.
A clinical observership is a period of time where a doctor observes another doctor or clinical team in a non-active capacity. The most common reason for this is to permit doctors from other countries to familiarise themselves with the Australian health care system and gain exposure to patients. Most such placements last around 4 to 8 weeks.
How do I find a Clinical Observership?
If you are an international medical graduate a clinical observership is not only a great opportunity to gain exposure to the medical system in Australia but it may provide you with an opportunity to make connections with potential future employers. So it’s not surprising then that clinical observerships are highly sought after.
Most clinical observerships tend to be arranged through personal connections. For example, you may know a senior clinician in a hospital who is able to arrange a clinical observership for you. Some hospitals may offer formal observership programs such as Northern Health in Melbourne, in which case the criteria for gaining an observership is quite high.
Be aware that the hospital may be using observerships to test out potential employees. So it’s probably best to have some grounding in what sort of things employers look for in medical officers before embarking on an observership.
Where is the best place for medical Intern pay in Australia?
In order to work out where the best place to work as a medical intern in Australia is we would need to take a number of factors into consideration including remuneration, career opportunities, work conditions, the desirability of location and cost of living.
Coupled with this Western Australia has some very nice places to live and has recently become a far better prospect for the cost of living, in particular renting and buying a house, since the decline in the mining boom that grossly affected housing prices there.
Where is the worst place to work for medical Intern pay in Australia?
If we were to use the same factors that make Western Australia the best place to work in Australia then New South Wales, in particular, Sydney would be easily the worst place to work as a medical intern in Australia. The pay rates for interns in NSW are the worst in the country and it doesn’t get better as you progress as a trainee. And, of course, Sydney is the most expensive city to live in in Australia.
But it’s not all bad. New South Wales has a lot of training opportunities and Interns in NSW are offered a 2-year contract, whereas Interns in other parts of the country are only given one year. This makes a great difference as it can take the pressure off in your first year because you are not worried about impressing your employer to get another job the following year.
Related Questions
Exactly how much can medical interns make from shift-work and overtime?
Whilst the base salary of an intern in Australia is somewhere between $68,000 and $79,000 AUD it is possible to do considerably better than this. Most interns are required to do a level of overtime and what is called shift work (work outside the normal hours) both of which are paid at a higher level than normal work. For example, most overtime (work in excess of 40 hours) is paid at double time in Australia.
So you can see that that base salary can improve quite significantly. But of course, it also means you are working longer hours, which may not necessarily be a good thing.
How much does a Resident Medical Officer earn?
A Resident Medical Officer is someone who is at least a year more senior than an Intern. In their first year, a Resident Medical Officer will earn considerably more money than an Intern. For example in NSW interns earn a base salary of around $66,000 AUD and first-year residents earn a base salary of around $77,000 AUD.
Do corporate Interns ever get paid?
Corporate internships are sometimes paid. Using non-paid employees to do the work of employed workers can get employers into trouble with regulator authorities, particularly in countries like Australia. So generally corporate internships that are of longer duration do tend to get paid.
Is there somewhere I can find out more information about pay rates for doctors in Australia?
Interestingly there is no one place to find out about doctor pay rates across the country. We have written a blog post that summarizes the pay rates for interns across Australia here and we hope to have the time to summarize the rest for you. Check back regularly.
We were all appalled to read yet another blog post about yet another trainee doctor badly treated on a regular basis by the medical culture system that we all belong to. Who are we? A group of clinicians who aggregate around an idea that we can be innovative in medicine and bring solutions to the table. Our thoughts naturally turned to rage as we reflected on the story of Dr. Yumiko Kadota, a plastic surgical trainee at Bankstown-Lidcombe hospital, who was forced by her medical culture to be on-call for 180 hours straight amongst a litany of appalling work practices.
But then we thought about it more deeply and decided as a group we should turn our thoughts to the problem. The problem is how do we change the terrible and sick culture in medicine and healthcare more generally? One issue that is readily apparent is that, if there was an obvious solution, someone would have found it by now. The traditional approaches of policy changes and awareness campaigns and training have not been particularly effective. Amongst our creative solutions to solving the problem with the medical culture we propose:
closing the accreditation gaps to ensure that all trainee doctors are subject to external accreditation
treating trainee doctors more like pilots
having clear rules and a chain of responsibility for wellbeing issues such as fatigue
using social networks to share good and bad information about trainee posts to shine a light on poor hospital practices
rewarding good teachers and supervisors with more trainees and taking trainees away from the poor ones
consultants giving up some of their pay in a genuine effort to demonstrate respect for trainee doctors and fix some of the systemic problems with work conditions
Our group is broad and comes from a range of backgrounds. Holding expertise in both medicine and other fields. This blog post was a joint effort by several individuals. We would love to tell you who each member was that contributed. But I am sure that you will understand why many of our members wish to remain anonymous. So. Here is a more in-depth look at some of our creative proposals
1. Close The Accreditation Gap.
One of the key issues in Dr. Kadota’s case is that even though she is a trainee doctor, she is not a doctor actually in training. Paradoxically and perversely Dr. Kadota is in training to become a doctor-in-training. This situation is due to bottle-necks in certain popular training programs, like plastic surgery. It leaves a situation ripe for exploitation where trainees in unaccredited roles can be exploited by hospitals because they are not officially backed up by the college and the hospitals know that there are many willing trainees ready to replace them. It creates a situation of what is commonly called “service roles”, which can also be interpreted as roles where you don’t get taught.
The solution is for the colleges to take formal responsibility for unaccredited trainees in their specialty areas. To ensure that there is a level of standard for the training and welfare of these trainees. If the colleges are unable or unwilling to do so then other authorities such as the Health Education and Training Institute, which in NSW already accredits hospitals for intern and resident teaching should be brought in to set and monitor standards.
2. Acknowledge That Fatigue Impacts Performance & Utilise a Pilot Style Regulation of Doctors.
The aviation and other transport industries have strict rules in place enacted by CASA regarding how much sleep someone needs to have in order to operate a heavy vehicle that may also be carrying passengers. This is based surrounding a strong research base acknowledging that fatigue can have a detrimental impact on concentration and performance and at some levels, as great as being intoxicated.
Why should doctors not also be viewed in the same way? Medicine is a challenging job in that every decision can potentially affect the lives of their patients, themselves, or their colleagues. Fatigue can impact medication prescriptions and errors, surgical errors, patient identification errors. It can also impact a doctor’s well-being, impact their families and result in car crashes (and deaths) on the way home from shifts. Fatigue has the potential to kill and can be costly for organizations.
Recent reports have highlighted the power imbalance that Specialty trainees, especially those in niche fields of medicine, have been treated poorly without representation of a college. They should be treated and respected as rare and valuable resources not flogged mercilessly because there are not yet accredited trainees or because there is a shortage of them. There are other ways of covering a specialty roster. Many hospitals in Australia do not have a 24-hour plastic surgery trainee doctor on call. Some don’t even have a plastic surgeon at all. It is time to review rostering and to think laterally about how to ensure safety for patients and doctors.
3. Adopt a Chain of Responsibility Approach.
Following on from the linkage to the airport industry. The heavy trucking industry has adopted legislation that makes everyone in the chain potentially responsible for adverse outcomes. If you put pressure on a truck driver to cut corners in order to save money for your business and that leads to unsafe driving you can be held criminally accountable for your action.
We suggest making those in charge of rosters responsible in some way for supporting poor roster practices. It is not as if there have not been guidelines in place for some time to say what is and what is not acceptable. The AMA’s National Code of Practice for Safe Working Hours was developed in 1999 and significantly redeveloped and refined since then. We have a tool. We can use it.
If a senior doctor authorizes an unsafe roster then there should be a penalty to both that doctor as well as the hospital. Be it financial or some other sanction. Heads of the Department will soon stop approving such rosters and either fight for change, advocate for resources or quit their role because they are not getting enough support from the hospital general manager. This pushes the problem higher up the food chain until someone decides to intervene.
As we have noted above. There is clear evidence that fatigue affects the health of the person with fatigue. There are many stories of doctors crashing their vehicles driving home from work. Medical trainees with fatigue are three times more likely to have an injury related to a sharp instrument like a needle-stick injury. Fatigue in pregnancy can increase the risk of miscarriage, premature labour, and low birth weight. There are many more documented effects of fatigue on the health of the person with fatigue. We know it is bad for doctors. We also know that doctors have higher rates of depression, anxiety, and suicide than the general population.
The evidence in medicine is less clear whether fatigue leads to unsafe care or medical error. But what we do know is that the effects of working continuously for 18 hours are equal to having a blood alcohol concentration of 0.05g/% and that 24 hours to a BAC of 0.10g/% or twice the legal driving limit in Australia. The RACS publication also states that approximately 33% of surgical errors are attributed to fatigue or an excessive workload.
Yet there are paradoxes, the Royal Australasian College of Surgeons RACS also recommends that a workweek of 65 hours is ideal for surgical training. This is based upon a review of the evidence and an acknowledgment that a certain amount of hours are required to develop to the level of expert. This takes into account factors such as working enough hours to gain the necessary skills to be a surgeon.
So what does that mean for patients?
Potentially that the doctor who is about to operate on you has not slept for 24 hours. Potentially that there is an increased risk of an error being made during your operation.
So what can patients and their families do?
When the doctor is explaining the operation, the benefits and risks of having the operation, or not having the operation, consider asking them whether they are in the high-risk fatigue category. Perhaps patients can help empower doctors to speak up.
If a patient declines a treatment because they believe that their doctor is not safe to operate and no other trainee doctor is available to take over, then more senior doctors would have to be brought in (if urgent) or if not urgent the issue placed on hold until there is a well-rested doctor available.
Dr. Kadota’s story highlighted a situation where there was pressure to move patients through the system. Not necessarily because of any clinical urgency, but because other KPIs demanded that the plastic surgical trainee is woken for non-urgent matters.
This situation would not arise in many of the hospitals in Australia. Because in many hospitals in Australia there is no 24-hour plastic surgical service.
5. Address The Supply and Demand Problem.
Part of the problem highlighted in Dr. Kadota’s case is a demonstration of the issues of supply versus demand. Doctors are in relatively short supply in certain areas and specialties. The short supply means that doctor-impairment is tolerated by hospitals and society (i.e. a drunk/fatigued/depressed/burnt-out doctor is better than a no-doctor).
Another part of the problem is the ‘naturality-of-outcomes’ in medicine – how is a member of the public meant to differentiate whether death or medical complications arose from ‘bad luck’, or an ‘impaired doctor’ who missed something? They can’t, and therefore the prospect of doctor impairment is never considered.
Finally, there’s the culture of obfuscation. When was the last time you as a doctor filed an incident report after discovering another doctor’s mistake, or noticing another doctor was tired/fatigued/emotional? Aviation, rail, and other transport industries have “fatigue-leave”, “normalised-incident-reporting”, supporting-fitness-for-work programs, and actively address the ‘authority gradient’ that exists between hierarchy, for eg. Captains and First Officers.
While the determinants of why bullying and burnout occur in medicine are complex, medicine like any industry obeys market forces across human needs. Success may lie in understanding that market and making the nurture-of-doctors a market commodity.
This can be done by better demonstrating that doctors who are well and cared for have better patient outcomes; have higher patient throughputs; save money, and improve patient satisfaction.
6. Alternative Models of Care
Following on from the above point. There are plenty of models in health where other doctors and other health professionals can take on some or all of the roles of a particular doctor who is in short supply.
This can be as simple as changing the process for who takes the first call from another doctor.
In Dr. Kadota’s case, she was apparently being woken in the middle of the night to receive calls about booking outpatient appointments. This function could easily be handed off to an administrative role.
Some teams will utilize experienced nurses to take the first call and triage the need and priority. A great example of how this happens are stroke teams and mental health teams.
This can be a fantastic opportunity for another member of the health care team to upskill in this role.
But of course, we have to be careful that we are not pushing the problem onto another part of the healthcare team by ensuring that everyone receives decent support and working conditions.
7. Use Social Media and Networks.
Sites like messly enable trainee doctors to connect and share information about hospitals. The good the bad and the ugly. Call it a name and shame exercise if you will but since the United Kingdom started asking its medical graduates whether their medical school did a good job in preparing them for internship (called foundation year in the UK) the satisfaction reports have gone up significantly over time and some pretty prestigious institutions were forced to lift their game.
One can imagine for example a public version of TripAdvisor for rotational hospitals where we get to see what the “well-appointed family-friendly 3 bedroom unit” truly looks like before they get sent there. The public can also see what’s happening and hold the system accountable.
8. Mass Exodus?
Miko’s story has resonated strongly with one eminent specialist in our group. This person has been working as a specialist for a few years but has become increasingly disillusioned with the hospital system that does not support its workforce.
Workforce cuts meant already overburdened staff having to take up additional work, compromising patient care. The staff had attempted to highlight the results of this, ranging from patient harm due to inadequate resourcing to the insidious deteriorating physical and mental health of the members of the team. Incidents reports were submitted, discussions were had at the appropriate committees, and even letters were written to management and the district CEO. Yet there was never a response, only non-responses or moves to hold the issue to the next meeting “let’s put a pin in it” when it was not discussed.
Miko’s treatment at this hospital is reflective of a wider systemic disease in the public (and private) hospital systems: the pursuit of KPIs or profit prioritized over the welfare of staff and patients. But more concerningly is the indifference of the healthcare system (Department of Health, State bodies, District Boards, and Hospital Management) to recognizing this disease and curing it. Failure to address this hurts staff and ultimately patients.
The core business of hospitals and the healthcare system is to care for the unwell, return them to health, and keep them healthy. This was the goal of the specialist in our group when they took up their specialist position in the public sector. After a few years, it was clear to the specialist that the hospital system disincentives and does not empower staff at the coal face to improve or address concerns or problems that are occurring. For these reasons, the specialist felt they had to leave as they were powerless to be able to change the system to the benefit of their colleagues and patients. Change that would have prevented Miko’s story can only come from within the health system. External pressures may drive this – Department of Health directives, The Media exerting pressure or Health Board Director prosecutions for failure to appropriately implement workplace health and safety procedures for staff.
Whatever the drivers are, it will be management and health care providers who create and implement solutions that support staff to work safely and innovate for the patients we serve.
Let’s hope it does not come to a mass exodus of medical staff leaving the system.
9. Make Supervision a Formal Credentialing Matter.
Senior medical staff has to go through an appointment and vetting process to get a role in any hospital in Australia. This process considers their training, qualifications, experience, and expertise and determines what they are and are not permitted to do. Sometimes referred to as a scope of practice. It’s generally about what sort of patients they are allowed to have admitted under their name, as well as what treatments, investigations, procedures, and surgeries they can conduct.
Nowhere in this process is there a consideration of their ability to teach, lead, supervise or just treat more junior staff members fairly. Having a trainee under your supervision should not be a right it should be earned. We should start by demonstrating this by not making the right to supervise and have trainee doctors in your team an automatic privilege.
10. Give The Best Teachers and Supervisors More of the Trainees.
If a senior doctor is unable to provide good supervision to a trainee, chances are they are not getting the best out of this particular valuable resource. Give more trainee doctors to the best supervisors and teachers in the hospitals. Let them lead “super-teams” that get the work done in a challenging but rewarding manner. Those supervisors who demonstrate poor supervision skills should be left to do the work of the consultant and the trainee.
There are many potential outcomes of this scenario. All of them are likely to lead to better patient care. In one. The poorly performing supervisors up their game through training and coaching and regain their trainee doctors. On the other, the poorly performing supervisors leave the hospital and their places are taken over time by new consultants who have been trained to be the best supervisors by the best supervisors.
11. Senior Doctors Forfeit a Pay Rise To Fix The Mess
Personal Opinion By Anthony Llewellyn
In some states of Australia, the Award for trainee doctors is pretty reasonable. In Victoria, for example, trainee doctors get access to annual leave, as well as study leave, exam leave, and even have access to a professional development fund.
In NSW however, where Doctor Kadota worked, we pay our trainee doctor’s the worst salaries in the country and we have an Award with all manner of antiquities and outdated conditions because it has not been updated for at least 4 decades. Trainee doctors struggle to get access to leave to study and prepare for exams and being sent to a hospital 150 kilometers away is not necessarily considered a rotation, where you get additional payments to support the fact that you are away from home. 35-year-old professionals (that’s what a trainee doctor is) are often offered an un-family friendly one-bedroom unit for their 6-month rural opportunity when they are living in a 4 bedroom house back at home with their spouse 2 kids and pets.
Every time there has been an attempt to bring in sensible and civilizing new conditions to the Junior Doctors Award in NSW it has been met by resistance. The most recent attempt to fix a problem was a simple proposition that we should recognize that specialty trainees are in fact specialty trainees and should be paid as such. It met heavy resistance from NSW Health and ended in a farcical status quo.
The main reason for this blinkered intransigence. Money. Every proposed award change is run over with an economic pen to see how much it will cost the bottom line. So that instead of making actual improvements to working conditions every year all that happens is a blanked percentage pay rise.
As a consultant who works in NSW Health, I value the work that the trainee doctors do. I could not do my work without them. I get paid well enough. Well enough that I could and would give up my next annual salary increase if I knew and it was promised that this would go to fixing up some of the problems that trainee doctors experience.
If you are a doctor from another country entering Australia. Unless that country is a country like the United Kingdom or United States, you are probably a little confused by what the specialist medical colleges are and do. Even trainee doctors in Australia get confused about the medical colleges.
Don’t worry we have you covered in this guide. We even give you the list and links to all of the Colleges with a bit of an explanation of what sorts of fields of medicine they cover.
What are the specialist medical colleges?
The specialist medical colleges are member based and training organizations that generally cover a certain aspect of specialist medical training in a country. The colleges developed historically in the English medical system from trade guilds and so are common in countries which developed their medical systems from the English system, for example, United States, Canada and Australia. The colleges have official status and a license to uphold the medical standards in their area of medicine. Examples of specialist medical colleges are:
Whilst colleges and universities both provide postgraduate education. Colleges generally differ from universities in two main ways:
Colleges apply an apprenticeship model of training, i.e. you work under supervision of an expert in the specialty. Whereas, universities apply other models of learning. This difference relates back to the time when colleges emerged from a number of other trade guilds.
Once you have completed college training you are generally invited to become a member of the college where your ongoing professional development is served and where you are expected to teach and supervise new trainees. Whereas, once you complete a university degree you may be asked to join the alumni but there is no expectation to take an active role in the university nor teach other new students.
The specialty medical colleges generally cover 2 components of the medical training continuum. The first being postgraduate medical education – the training required to become recognized as a specialist. The second being ongoing or continuing professional development (CPD), which has historically been known as continuing medical education (CME). This is where the colleges act to support and monitor the standards and currency of current specialists.
A short list of the 16 Australian Specialist Medical Colleges (we include the College of Dental Surgeons here):
Australian College of Sports and Exercise Physicians (ACSEP) www.acsep.org.au
College of Intensive Care Medicine of Australia and New Zealand (CICM) www.cicm.org.au
Read on further for more details about these colleges and what they do.
Now that you know what a specialty medical college is. Let’s talk more about some of the confusing points of colleges. What types of colleges there are in Australia and importantly how to work out which college is the right college for you.
Alternative Approaches to Medical Specialty Colleges.
In other countries and health systems medical specialist training is delivered through universities and other educational institutions and continuing professional development is monitored by regulatory authorities, medical boards and licensing authorities. When doctors from these countries they can sometimes be confused about what a college is or does.
Hybrid Models.
To add further to the confusion in some countries there is overlap between the role of the specialty medical colleges the universities and other medical authorities. Canada and the United States is a good example of this. In these countries much of the postgraduate training is delivered via university programs but overseen by specialty medical colleges.
In the United Kingdom the role of the colleges as training providers has also shifted in the last decade or so, with the college role in providing training and determining specialist qualification being reduced.
The Status of the Specialty Medical Colleges in Australia.
In Australia the specialty medical colleges remain very powerful. With the possible exception of general practice (which is a specialty by the way) the specialist medical colleges generally have the oversight of and organize much of the specialty training that occurs in this country as well as continue to monitor the continuing professional development of their members (called Fellows).
What are the Medical Specialty Colleges in Australia?
Something that should be pointed out at this point is that most (but not all) of the specialty medical colleges in Australia are also the same college for the country of New Zealand. This has the handy advantage for Fellows of these particular colleges being able to be recognized and work in either jurisdiction. You will notice most colleges either refer to themselves and the “Australian and New Zealand College of”… or “Australasian College of”, for this reason.
See below for a full list of the current Medical Specialty Colleges in Australia along with links to their websites.
On each College home page, there is usually an easily found link in the menu bar for prospective trainees, as well as international specialists looking for information about the specialist assessment process. We also have direct links to the specialist assessment pages for SIMGs here.
Our data sources for the table below come from the Colleges themselves as well as the latest available Medical Board data which you can find here, as well as health workforce data, from the Federal Government. You can find the homepage for this data collection here.
Number of Fellows: 19,673 Fellows (Aus &NZ) – source RACP.
Specialist Numbers: 12,672 Adult Medicine, 3,621 Paediatrics, 439 Palliative Medicine, 198 Addiction Medicine, 137 Sexual Health, 452 Public Health Medicine, 591 Rehabilitation Medicine, 308 Occupational and Environmental Medicine –source Medical Board Australia.
Main Post Nominals (FRACP).
Actual total slightly higher due to other programs offered, some of which are jointly run with other colleges.
The RACP is one of the biggest Colleges. It also the most complex in terms of training programs. There are about 37 training programs. Fellowship of the RACP covers a range of aspects of specialty medical training, with a focus on Adult Medicine and Paediatrics
If you are struggling to work out where your field of medicine fits, chances are it fits within the Physicians College.
In the two main groups of Adult Medicine and Paediatrics and Child Health there are many subspecialties including General Medicine and General Paediatrics as well as things like Cardiology, Infectious Diseases, Geriatrics and Neonatal Care.
The RACP also covers 3 Chapter Training Programs in Addiction Medicine, Palliative Medicine as well as Sexual Health Medicine which you can enter after doing your Basic Training with the RACP or via training with another college.
Finally the RACP also provides 3 Faculty Training Programs in Public Health Medicine, Occupational and Environmental Medicine and Rehabilitation Medicine. Again, you can either enter into these after Basic Physician Training or by completing other prerequisites.
Fun Fact: The RACP even covers Dermatology for New Zealand!
Number of Fellows: 6,842 Total. Comprising: 2,362 General Surgeons, 1,779 Orthopaedic Surgeons, 624 ENT Surgeons, 573 Plastic and Reconstructive Surgeons, 568 Urologists, 325 Neurosurgeons, 246 Vascular Surgeons, 239 Cardiothoracic Surgeons, 126 Paediatric Surgeons (Aus & NZ) – source RACS.
Specialist Numbers: 2,214 General Surgeons, 1,577 Orthopaedic Surgeons, 547 ENT Surgeons, 516 Plastic and Reconstructive Surgeons, 508 Urologists, 292 Neurosurgeons, 256 Vascular Surgeons, 212 Cardiothoracic Surgeons, 106 Paediatric Surgeons – source Medical Board Australia.
Post Nominals (FRACS).
Fellowship of the Royal Australasian College of Surgeons is one of the most highly sought after fellowships. Entry into any one of the 9 specialty training programs is highly competitive.
The subspecialty areas are: Cardiothoracic Surgery, General Surgery, Orthopaedic Surgery, Otolaryngology, Head & Neck Surgery, Paediatric Surgery, Plastic & Reconstructive Surgery, Urology, Vascular Surgery, and Neurosurgery.
Outsiede of the Royal Australasian College of Surgeons Building in Melbourne, Australia Attribution: Canley, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons
Number of Members (includes trainees and other non-Fellows): 40000+ – source RACGP.
The total number of General Practitioners in Australia 34,654 – source Medical Board Australia.
Post Nominals (FRACGP).
The RACGP is by far and away the largest College in Australia. It is also one of the few colleges which is not involved in training within New Zealand. However, if you do have the FRACGP, you will receive reciprocal recognition in New Zealand.
General Practice is recognized as a specialty in Australia. In other countries this specialty may be referred to as Family Medicine, a Family Physician or Primary Care
Training to be a GP is conducted via a few different pathways. The largest one is the Australian General Practice Training Program, which is separate to the RACGP.
So the RACGP is a little different to other colleges in that, whilst it still sets training program requirements and conducts examinations, the training itself is done externally to the college.
The RACGP also provides an alternative training program where with a small amount of additional training you can be recognised as a rural GP (FARGP).
Number of Specialists: 4,409 – source Medical Board Australia.
Post Nominals (FRANZCP).
The RANZCP is one of the last true generalist specialist colleges in Australia. Its training program runs for 5 years and includes mandatory training in Adult Psychiatry, Consultation-Liaison Psychiatry (General Hospital Psychiatry), Child and Adolescent Psychiatry as well as a range of other types of experiences and assessments.
Towards the end of training, trainees can elect to undertake Advanced Training in a certain area of Psychiatry, including Child and Adolescent, Consultation-Liaision, Adult Psychiatry, Old Age Psychiatry, Neuropsychiatry, Forensic Psychiatry and Psychotherapy, however all trainees emerge from the program considered competent to work in all fields of the specialty.
It is expected that the position on generalism in Psychiatry will change in the not too distant future.
Number of Fellows: 6,000 specialist anaesthetists and 460 pain specialists (Aus & NZ) – source ANZCA.
Specialist Numbers: 5,793 Anaesthetists, 383 Pain Medicine – source Medical Board Australia.
Post Nominals (FANZCA).
ANZCA ANZCA is responsible for the training, examination and specialist accreditation of anaesthetists and pain medicine specialists in Australia and New Zealand. In any given year there are about 1500 trainees undergoing training accredited by ANZCA in Australia and New Zealand. The College also has a number of trainees in Singapore, Malaysia and Hong Kong.
Specialist Numbers: 3,098 – source Medical Board Australia.
Post Nominals (FACEM).
At 35 years ACEM is one of the newer colleges in Australia. It is also one of the first colleges in the world that represented the specialty of emergency medicine that emerged (pardon the pun) in the 1970s from hospital casualty department medicine.
The Association of Casualty Supervisors of Victorian Hospitals (ACSVH) was the first body in Australia to focus on Emergency Medicine. Its formation followed a 1973 report on the Royal Melbourne Hospital’s Casualty Department and observations of similar facilities in Western Australia, the USA and the United Kingdom.
The total number of General Practitioners in Australia 34,654 – source Medical Board Australia.
Post Nominals (FACRRM).
The Australian College of Rural and Remote Medicine is one of two colleges accredited by the Australian Medical Council (AMC) for setting professional medical standards for training, assessment, certification and continuing professional development in the specialty of general practice. It is the only College in Australia dedicated to rural and remote medicine, and is active in supporting junior doctors and medical students considering a career in rural medicine. ACRRM’s training approach is quite different from most other colleges and based partly around modularised learning. ACRRM Fellows receive full vocational recognition for Medicare General Practice Items and are not just restricted to working rurally, they can practise unsupervised anywhere in Australia.
As a relatively new and small college ACRRM tends to be particularly welcoming to International Medical Graduates.
However, the FACRRM has more limited recognition overseas in comparison to the FRACGP.
Specialist Numbers: 2,265 – source Medical Board Australia.
Post Nominals (FRANZCOG).
RANZCOG is the College that deals with the specialty of womens’ and maternal health.
RANZCOG has recently recognised 5 subspecialty fields within its specialty area: Gynaecological oncology, Maternal-fetal medicine, Reproductive endocrinology and infertility Ultrasound, and Urogynaecology.
Specialist Numbers: 2,375 – source Medical Board Australia.
Post Nominals (FRCPA).
The RCPA represents Pathologists and Senior Scientists (working in medicine) in Australasia. Its mission is to train and support pathologists and to improve the use of pathology testing to achieve better healthcare.
It is novel as a college in that it trains non-medical professionals as well.
There is some degree of overlap in training and representation with the RACP. Particularly in relation to the areas of haematology and microbiology. Post fellowship diplomas are also available in anatomical pathology, chemical pathology, clinical pathology, forensic pathology, general pathology, immunopathology and genetic pathology.
A Faculty of Clinical Forensic Medicine also exists within RCPA.
Number of Fellows: 1000+ (Aus & NZ) – source CICM.
Specialist Numbers: 1,096 – source Medical Board Australia.
Post Nominals (FCICM).
The College of Intensive Care Medicine is the body responsible for intensive care medicine specialist training and education in Australia and New Zealand. The College offers a minimum six-year training program, in both general and paediatric intensive care, with a number of assessments, culminating in the Fellowship of the College of Intensive Care Medicine (FCICM). The College has over 1000 Fellows throughout the world.
The College of Intensive Care Medicine was established in 2008 and formally took over the responsibility for training and certification of intensive care specialists from the Joint Faculty of Intensive Care Medicine (RACP & ANZCA) on 1st January 2010.
Specialist Numbers: 633 – source Medical Board Australia.
Post Nominals (FACD).
The ACD is the peak medical college accredited by the Australian Medical Council for the training and professional development of medical practitioners in the specialty of dermatology.
Post Nominals (FRANZCO). The Royal Australian and New Zealand College of Ophthalmologists (RANZCO) is the medical college responsible for the training and professional development of ophthalmologists in Australia and New Zealand.
Number of Fellows: 503 (Aus, NZ and Hong Kong) – source RACMA.
Specialist Numbers: 355 – source Medical Board Australia.
Post Nominals (FRACMA). The Royal Australasian College of Medical Administrators (RACMA) is a specialist medical college that provides education, training, knowledge and advice in medical management. Recognised by the Australian and New Zealand Medical Councils, it delivers programs to medical managers and other medical practitioners who are training for or occupying Specialist Leadership or Administration positions. Whilst you generally do not require a Fellowship in Medical Administration to work in a leadership role, RACMA is the only college-based training program where you can become a Fellow in the Speciality of Medical Administration.
RACMA also has significant options for recognition of prior learning.
Specialist Numbers: 158 – source Medical Board Australia.
Post Nominals (FACSEP).
ACSEP is the professional body representing Sport and Exercise Physicians and Sport and Exercise Medicine in Australasia. Sport and Exercise Physicians are committed to excellence in the practice of medicine as it applies to all aspects of physical activity. Safe and effective sporting performance at all levels is a major focus. Alongside this is the increasing recognition of the importance of exercise in the prevention and treatment of common and often serious medical conditions, such as arthritis, heart disease, diabetes and many cancers. The goal of all Sports and Exercise Physicians should be to facilitate all members of the community to enjoy exercise safely to 100 years and beyond, knowing that physical activity provides them with the ‘best buy’ to prevent chronic disease.
Specialist Numbers: There are 177 Oral and Maxillofacial Surgeons according to the Medical Board Australia.
Post Nominals (FRACDS(+/-OMS)).
The RACDS is over 50 years old and Fellows have been providing a broad range of activities to enhance the professional development of both general and specialist dentists through individually mediated studies, examinations and continued professional development. It is responsible for the RACDS OMS Training Program.
The OMS Training Program is designed to provide trainees with sufficient theoretical and practical background to meet all current standards available in Oral and Maxillofacial Surgery in Australia and New Zealand.
Eligibility for this program includes the requirement to have both a medical and a dental degree and full registration in both specialties, as well as a year of general surgical experience. So becoming an OMFS surgeon is possibly the longest specialty training program in Australia!
How To Work Out Which College Is For You If You Are A Specialist International Doctor?
If you are from overseas it can sometimes be tough to work out how your particular specialty fits into the Australian system or in fact how your training may differ from what occurs in Australia.
Here’s an example, in the United States Child and Adolescent Psychiatrists train primarily within the field of child and adolescent psychiatry and probably learn more paediatric medicine than any other form of psychiatry. Whereas in Australia, you have to start out training in general psychiatry and only at the stage of Advanced Training do you undertake significant periods of study in Child and Adolescent Psychiatry.
This can have significant issues for child psychiatrists as much of their training won’t stack up against the program in Australia.
If you are considering working here as a specialist here are a few tips to consider when working out which college fits you:
There may be an obvious first starting point. For example, if your field is within the surgical domain, you are likely (but not always) to be covered by the Royal Australasian College of Surgeons. Exceptions might include Ophthalmic Surgeons and Dental Surgeons.
If you have worked generally for many years and are considered a specialist in your country. But you do not have a certificate or have not undergone a formal specialty training program or course. You are unlikely to be granted specialist status in Australia.
If you cannot work out where your particular specialty fits and it’s not surgically related it probably fits within the Royal Australasian College of Physicians and their many programs. Or as an alternative, it may be covered by General Practice.
You can actually ask the colleges. They will answer some basic questions before charging you to look at your specialist application. A question like “this is my subspecialty, do you cover it here?” should be answered free of charge.
How To Work Out Which College Is For You If You Are An Australian Trainee Doctor?
For Australian trainee doctors, there are many opportunities to inform themselves about the various specialty trainee options. Some of the things that you can do include:
making a list of specialties that interest you and maximising your exposure to them in medical school and your early days as a medical graduate by choosing electives wisely and being selective about any choices you have about hospitals and rotations
reviewing information on the college websites
attending careers sessions
talking to actual trainees doing the role (this is a great tip as it gives you a very authentic appreciation of what it’s like to work and train in a particular specialty)
When considering specialty training it’s important to consider the “80:20” rule. Many doctors are attracted to certain specialties because of their interests in rare conditions or niches within the specialty. You may well end up being the one right-ventricular surgeon in Australia. But you probably won’t and you will have to go through a lot of steps to get there if you do.
It’s best to consider what’s common about the specialty as both a specialist as well as a trainee:
What sorts of patients will you be regularly seeing?
What sort of hours will you work?
Where will you work?
Is research or teaching a regular component of the role or a rarity?
The classic example is Endocrinology. Whilst there are many fascinating conditions in the field of endocrinology. If you are not interested in looking after at least some people with diabetes mellitus you should probably choose something else.
Below are the rest. More information about these other colleges coming soon.
The History of Medical Colleges
In Europe in the 18th century, unqualified people performed certain restricted medical tasks that other qualified practitioners viewed as quackary. This included procedures, such as “cutting out stone” a (a surgical incision to remove urinary calculi from the bladder) or “couching” (dislodging cloudy cataract lenses using pressure or a surgical instrument and pushing it to the back of the eye) as well as bone setting.
The answer to this question is a little more complex than one might think. We have already discovered that there are 15 colleges. 16 if we include the Dental College, which we really should as they include the oral-maxillofacial surgeons. But we know that there are then a range of subspecialties and other programs housed within some of the colleges, in particular the RACP and RACS. The Australian Medical Council in its role of accrediting specialty training programs (see below) currently recognises 25 programs. This number captures all the colleges, as well as the additional programs that the RACP offer and two different programs for Intensive Care Medicine. The former the Joint Faculty for Intensive Care Medicine is now a defunct program and will be removed at some point in lieu of the more recently established College of Intensive Care Medicine. This is an example of how college evolve over time and new colleges arise. See below. At last count according to the Medical Board of Australia there were around 64 recognised subspecialties in Australia. But this doesn’t even compare to the United States, where the Association of American Medical Colleges lists 131 specialties.
How many specialists are there?
According to the Medical Board of Australia. As of June 2022, there were 78,887 medical specialists registered, covering a total of 84,602 specialty field recognitions. The latter is larger than the first as some specialists have dual specialist endorsements. For example, an Anaesthetist may be endorsed for both anaesthetics and pain medicine.
Is General Practice a Specialty?
In one word. Yes.
What was the First Specialty COllege?
Founded in 1518 by a Royal Charter from King Henry VIII, the Royal College of Physicians of London is the oldest medical college in England. It continues to play a pivotal role in raising standards and shaping public health today.
“In the 1500s medical practice in England was poorly regulated. Many ‘physicians’ were working with no formal training or knowledge, and almost certainly killed as many patients as they cured. The leading physicians of the early 16th century wanted the power to grant licenses to those with actual qualifications and to punish unqualified practitioners and those engaging in malpractice.
A small group of physicians led by the scholar Thomas Linacre petitioned King Henry VIII to establish a college of physicians on 23 September 1518. An Act of Parliament extended its powers from London to the whole of England in 1523.
Originally called the College of Physicians or the King’s College of Physicians, it only gradually became known as the ‘Royal College of Physicians of London’ during the 17th century. It was only with the restoration of the monarchy, that the RCP started referring to itself consistently as ‘royal’. But from the very beginning its members found their patients from the highest levels of society.
– Royal College of Physicians “Our History”
What was the Second College?
The second College in England was the “Company of Barber-Surgeons”, which was established in 1540. It formed out of a trade guild and a London Livery Company that apprenticed and examined trainees within the City of London. As the name suggests, what we now refer to as the medical specialty of surgery arose out of those tradespeople who earned their living from performing haircuts and beard trims and shaves. This makes sense as these tradespeople worked with sharp objects that were good for cutting things other than hair. So its likely that some developed skills at other useful forms of cutting. Initially the barber members of the guild were the most senior members but in time the surgeons became more respected and sought to break away and establish their own identity.
Who checks on the Colleges?
The Australian Medical Council is the body that checks the quality of the medical specialty colleges. Amongst other things they check both on the quality of the specialty training program as well as the continuing professional development program for existing college members. Yes the one that also accredits Medical Schools in Australia and New Zealand as well as prevocational training programs and assesses International Medical Graduates through the standard pathway. The AMC reports to the Medical Board of Australia, which has the final determination on college status.
Why are some called “The Royal…” and others not?
Most of the earliest colleges in Australia were off-shoots of their respective college in England. The specialist medical colleges in England all were given Royal Assent and the privilege of using the word Royal in the title. This patronage was continued through with most of the original colleges in Australia. You can tell which colleges have recently been established by virtue of the fact that they do not carry the word Royal in their title. For example the Australasian College For Emergency Medicine and the Australian College of Rural and Remote Medicine are relatively new colleges in Australia.
How do you start a college?
From a review of the 15 (or 16) medical specialty colleges and 64 or so specialties and subspecialties one might consider that there is not really the need for another college. But consider this. Medicine is always evolving and specialising. We can’t predict the future completely. But what we can probably predict is that over time certain doctors will probably organise as a new group around a set of health problems or ways of healing or working in health and eventually will want to establish their identity as a college. There are a couple of ways that this can work. One is to set up an entirely new college. Normally what happens is that a group of doctors who are already specialists in another college form a society first and over time build up membership, academic and professional development programs until the time that their is enough momentum for a new college. This is a difficult and arduous process. You can’t just call yourself a college and have your members start charging patients for their new specialty services. There is a process you have to go through to get a college recognised which involves an application to the Australian Medical Council. Even after you have convinced the AMC the Medical Board can refuse to accept your status and even then the Commonwealth does not necessarily have to agree that College members can access the important Medicare billing system for their patients.
The record shows that I have been a member of LinkedIn since 2010. This makes LinkedIn one of the longest-serving social networks that I have been a member of. LinkedIn started in 2002. That’s before Facebook (2004) which I have joined (before LinkedIn) and left a few times. So why should doctors use Linkedin?
Now I confess for significant parts of the past 9 years my LinkedIn profile got little attention. But I always saw the sense in keeping it. As a seasoned medical practitioner, past health executive and someone with decades of expertise in Medical HR I have come to view LinkedIn as a valuable and underrated social media platform and essential to my own career and a valuable tool for the careers of other doctors.
Here’s Why?
Doctors should use LinkedIn for Jobs because:
LinkedIn is generally accepted to be the social media platform for professionals.
Employers now look on Google to check information about doctor job candidates. LinkedIn profiles rank highly in Google.
Health employers are now starting to incorporate LinkedIn as part of their advertising and candidate identification strategy. So potentially not being on LinkedIn means you could miss out on a doctor job that would have been to your liking.
If none of that convinces you that LinkedIn is for doctors. Then consider this I have recently been getting approached by other doctors to help them with their LinkedIn profiles. These are doctors who never saw the value of the platform before and are generally not on many other social media platforms. Something must be up.
But wait there’s more. LinkedIn has other uses and if used properly can help you in other ways in your career.
Some of the other reasons why as a medical professional you should consider renewing your LinkedIn or starting a LinkedIn profile are:
1. LinkedIn is a great place for keeping all your career information.
Possibly the number one reason I like LinkedIn is that over time I have accumulated a lot of achievements in my career and LinkedIn is the vehicle by which I store these. For me. LinkedIn beats having to store multiple versions of your CV on your computer or dropbox and then going back over each of them the next time you need to submit your CV.
I always revise my CV each time I am asked to submit it. Which at the moment is about 10 times a year for various consultancy work and Board positions etc… LinkedIn is often my source of inspiration for when I get stuck with highlighting a certain skill or criteria.
2. LinkedIn for doctors is a great tool for controlling your online social presence and reputation.
LinkedIn profiles have high authority with Google and rank well on search. Just Google your name if you are on LinkedIn or someone else you know who is and you will see what I mean.
As a doctor you may not be concerned about your Google Search. But be aware that there are now a number of doctor review sites around where patients can express their opinion about you. And you won’t even know about it if you don’t go looking for it. Now you can spend time joining some of these sites and “claiming your profile” as well as establishing an active online presence. You can even develop your own authoritative website if you like. But that takes time. As Kevin.MD points out LinkedIn is not perfect but its a low risk, potentially low resource, high-yield action that you can take to protect your online presence.
With LinkedIn its still currently very easy to distinguish yourself from other doctors just by completing all of your profile. Most doctors just don’t bother to do it right which is good for you and bad for them.
3. LinkedIn Is Great For Building Strong Networks With Other Doctors As Well As Other Professionals.
We all know the saying “Its not what you know but who you know”. LinkedIn was built with that proposition in mind. And that’s an incredibly intriguing proposition for doctors who have taken years to memorize medical information. If you don’t have a great network yet, Linkedin is the best place to start. Doctors on Linkedin are generally very easy to connect with, even the experts. Especially, if you contact them in a genuine and non-spammy way, you’ll probably be able to add them to your network. This is something you could not have done a few decades ago.
4. LinkedIn Can Help In Creating A Personal Brand.
LinkedIn allows you to tell the rest of the medical world and others how exactly you see yourself. But this requires thought and activity. So if you don’t feel you have the time or need for this particular point feel free to skip to the next.
Personal branding is about building a reputation, authority and trust about you as a professonal. You are attempting to influence what people think about your when they see your content in a newsfeed or message. Will they click on the link you shared? Will they check out other people in your network and ask to connect with them as well?
The key success factor when building a personal brand is to create valuable content for your connections. You can do this by creating content yourself or just curating interesting information.
5. Doctors Can Use LinkedIn to Establish A Name As A Speaker Advisor Or Authority.
Doctors can sometimes earn additional income from speaking engagements or gain valuable connections or leads. If your name and face come up a lot in their newsfeed next to valuable information, you’ll be perceived as a trusted expert who might be asked to speak or review something.
6. Getting Relevant Information.
With regular use Linkedin becomes better at deciding what information might be relevant for you. They look at the keywords in your profile, your groups and your connections in order to decide what content to show. They are also more choosy than facebook about how much unsolicited content to show. So it doesn’t feel like you are constantly bombarded. About once a week I find a really interesting headline that leads me to a nice in-depth article on a topic of interest.
7. Getting Advice On LinkedIn From Other Doctors
Imagine you are thinking of applying for a new job at a hospital you are unfamiliar with but you don’t know if it’s a good idea. When the hospital says that the roster is normally one in five at full staffing do they actually mean it and how often are they fully staffed? LinkedIn can connect you with people currently working in this hospital who can clarify your questions. There are lots of situations I can think of where you could use Linkedin in order to get advice from someone who’s already undertaken the experience you are considering.
8. Being Found Online
These days it’s critical to be found on Google. Every day, thousands of patients, recruiters, industry professionals and students are looking for your services. So why make it difficult for them to find you? Google loves Linkedin – if you complete your profile and stuff it with the right keywords, you will not only be found when people are searching your name but also when they are searching for your specialty.
9. Landing Your Dream Job
This is probably the most obvious reasons for being on LinkedIn. Even if you are not a very active participant and get slightly annoyed by being spammed occasionally. Linkedin can be a great place to look for a new job when you need it. Traditionally doctor jobs are not be posted in the regular jobs section on Linkedin. However that’s changing. And if you are particularly looking for a creative or non-traditional career path. Whether that be a side gig or a permanent transition then LinkedIn will be a useful source of information for you. In addition, you can join groups targeting your specialty. There’s usually a job discussion section in these groups. There may be tips on the interviews or even early leads on job opportunities. For e.g. you might find out that a Neurosurgery Registrar has just left Hospital X early, leaving a sudden vacancy. Have a look there, then look who posted the job and connect with them.
7 Ways to Improve Your LinkedIn Profile As a Doctor
1. Upload a current, professional profile photo.
Profiles that include a photo are estimate do be more than 10 times more likely to be viewed. Or to put it another way. Not having a profile picture seems weird and is often equated to an incomplete profile. So get a photo. And yes I know that this is completely the opposite of the advice that I give about CVs. But its social media.
2. Be active on the platform.
Active profiles get more attention on LinkedIn. You can be active by joining and commenting on groups and occasionally posting your thoughts on a topic. You can use LinkedIn as a form of blog or you can link your existing blog to LinkedIn
3. Claim your LinkedIn tag.
Create a unique URL. This will make your LinkedIn profile appear unique and give the impression that you have taken the time to establish your brand (For example my LinkedIn is linkedin.com/in/drallewellyn). A custom URL makes your profile more professional and it also allows you to add a nice looking link to your business cards and CV or resume.
4. Use a customized headline.
If you don’t then each time you change jobs, LinkedIn makes your headline your your updated title (if you remember to update it). Think about using keywords that you want employers to find you for in your headline either on LinkedIn or Google. The headline of LinkedIn is important for Google search.
5. Keep your contact information up to date.
It’s simple, but oftentimes overlooked. Check the contact information section of your profile. Somethings on your LinkedIn profile are only visible to your connections. But contacts are visible to everyone.
6. Don’t share any contact information you’d prefer to keep private.
Its not kept private by LinkedIn.
7. Don’t forget to update your work profile when you change jobs.
Don’t be that person that everyone congratulates on their 12 year anniversary in a job they left 8 years ago.
Don’t forget to update your work profile when you change jobs. Don’t be that person that everyone congratulates on their 12 year anniversary in a job they left 8 years ago
Dr Anthony Llewellyn @careerdranthony
8. Make your summary personal.
This is a bit like your Career Goal Summary but with a bit more individual flair and passion to intrigue readers.
9. Fill out your profile as completely as possible.
There’s a reason why LinkedIn keeps nagging you to complete your profile. It improves your search on the platform. Also, as I’ve pointed out already, Linkedin then becomes a repository of all your career information for you to draw upon the next time your revise your CV or resume. Completing your profile can be a big task. But you don’t need to do it all at once. Just chip away at it over time.
So Why Don’t Doctors Join LinkedIn?
Most established doctors (we are talking specialists here) have until this time lived and worked in relatively small, geographically defined locations without having to shift too much in their careers. They have managed to be successful through word of mouth and connections. The average Consultant felt that they had no need to sell themselves beyond this local market.
It has also been generally held that doctors of a certain type are relatively similar in their skill sets (but not in their skill). For example what an orthopaedic surgeon does in Newcastle, NSW is likely to be similar to what one does in Perth, Western Australia.
Patients up until recent have had little insight into the quality of doctors and still struggle with what the economists call “consumer sovereignty”, which is the ability of a consumer to use their own knowledge to evaluate the cost of a product or service in a market.
But this is all changing. For one thing trainee doctors generally move around quite a bit and have to land several jobs before they are able to “settle down”. Patients are now getting access to insight and information about doctors through health review sites and there’s a lot more consumer sovereignty available now through Dr Google. Experienced clinicians are attempting to brand themselves in niches of medicine. And general practitioners are more regularly now referring to the internet with referring to a specialist.
In addition to the above many doctors may feel that their presence on LinkedIn serves very little direct benefit. As Dr Howard Luks points out he probably has not had very many patients come to him from LinkedIn and a lot of the contacts he has had have been nuisances. However, this is not the experience of every doctor and Howard himself balances out this problem by referring to the utility for LinkedIn to be a protector of online reputation.
What Benefits Have I seen From Being on LinkedIn?
Whilst I used to treat LinkedIn as a bit of a passive place to park my career profile. I have experienced more quality connections on the platform by being an active user. This has included interesting job referrals, connections to like-minded doctors across the world and clients and other opportunities and leads. Yes. You still get some annoying messages. Mainly from locum agencies. Which really wouldn’t be annoying if I was looking for a locum. But honestly we are talking once a week at best.
Related Questions About LinkedIn For Medical Professionals
How much time do I need to devote to LinkedIn as a Doctor?
Most LinkedIn users spend less than an hour a week on LinkedIn. But there are significant periods where they may be more active, for example, when looking for their next job opportunity. As I have pointed out above, LinkedIn is extremely useful if you want an online presence that you control but don’t have to spend a lot of time on.
It is however important to regularly review your LinkedIn profile. So you can’t completely forget about it. Otherwise when an employer looks you up and sees that LinkedIn says you are still working in the job you were doing in 2008 when your CV says otherwise they will probably think you are sloppy.
As a Medical Professional, Can’t I just use other social media platforms like Facebook?
LinkedIn is a bit different from the other social media platforms. For sure as Facebook has grown-up along with its audience its taken on a more “adult” look. But LinkedIn is still a more business like and less “social” platform than Facebook’s friends, groups and pages model.
You can’t really effectively record your CV on Facebook as comprehensively as you can on LinkedIn. And let’s face it the opportunities to be spammed and waste time are far higher on Facebook than LinkedIn.
From a marketing perspective, LinkedIn also have some value. Because one of its primary purposes is for being visible among and connecting with fellow professionals, including other health professionals.
Are there any alternatives to LinkedIn?
There have been attempts to set up social networks just for doctors, such as Doximity (haven’t used this) and SERMO (joined and found there to be no real community and no value). But given their narrow focus and LinkedIn’s edge in terms of being established in 2002 these platforms have struggled to be adopted.
I hope that by now I have convinced you that Linkedin is a great place to start your social media career as a doctor. Let me know how you have used Linkedin to your advantage in the comments section.
In my years I have reviewed tens of thousands of both doctor CVs as well as many other types of CVs and Resumes. I’ve gotten quite good at reviewing them quickly and determining who is and who isn’t a good prospect for a role.
A question I get asked a lot by other medical practitioners, particularly medical students and trainee doctors, about their CV is “Should I put a photograph on my CV?”. There are 3 main reasons why you should not put a photograph on your CV. 1. A photograph on a professional CV can be seen as pretentious 2. A photograph on a CV provides an opportunity for the reviewer to infer biases about you simply based upon your opinion. 3. A photograph on your CV distracts the reviewer from other important information.
There is also only one good reason why you should put a photo on your CV in my opinion.
The Only Reason You Should Put A Photograph On Your CV.
Let’s start with the reason why you should. It may seem fairly obvious. But there are some situations where the employer specifically requests a photograph on your CV. So if that is the case then you should obviously oblige.
Ok Now. What about the reasons why you should not put a photograph on your CV? Well the first reason is that Medicine is a conservative profession and if you ask interview panel members most will tell you that they feel that a photograph is a negative. Its just not what is expected and therefore too novel. The second is that the presence of a photograph can introduce the opportunity for biases to occur just based upon your appearance, which is less likely to occur when there is plain text on the page. And the final reason is that a photograph is likely to distract the reviewer from reviewing the other details of your CV. Which is quite crucial once you know how long it actually takes someone to review your CV the first time!
So my advice to doctors is to not put a photograph on their CV. There are too many possible minuses versus pluses to be gained.
So you may be wondering now. Why photos can distract or introduce biases. As well as possibly whether the situation might ever change in relation to photographs on your CV.
Why photographs are more likely to lead to biases
It is well established in psychology that one way that our attributions may be biased is that we are often too quick to attribute the behaviour of other people to something personal about them rather than to something about their situation. This is a classic example of the general human tendency of underestimating how important the social situation really is in determining behaviour.
When we tend to overestimate the role of person factors and overlook the impact of situations, we are making a mistake that social psychologists have termed the fundamental attribution error.
One of the best text-book examples of this integrates stereotyping: Imagine two doctor CVs both are exactly the same in terms of the training and experience they have had. One CV includes a photograph of a young looking female doctor. The other male doctor does not include a photo. Both doctors are both the same age. Which of the two doctors are the panel likely to stereotype as being “too inexperienced for the role”?
How long is spent looking at a CV?
The Ladders Survey is well known and well cited in the HR profession. In this survey the Ladders recruitment agency brought in a number of professional recruiters and recorded their actions as they reviewed candidate profiles online.
The results were stunning. On average seasoned recruiters were only taking 6 seconds to review a candidate’s resume and make a determination if they should be further considered.
When a candidate did add a photograph to their CV. Looking at this took up 20% of that valuable average 6-second time.
Pretty much everyone cites the Ladders Survey and the 6 second rule. And whilst we can debate whether its 6 seconds or perhaps a few more seconds. Lets say 8 seconds. If you talk to any doctor who is involved in mass candidate recruitment activities, such as annual medical recruitment. They will rapidly tell you that they have CV review honed to a fine art.
By the way one thing that most people have forgotten about the Ladders Survey is that they also found that professionally written CVs were seen to be 60% easier to read.
Update Feb 2019. Unfortunately the link to the 2012 report has been taken down. Ladders updated its eye-tracking report and reports that the average time for review has gone up slightly to 7.4 seconds.
The Implications of the 6-8 Second Rule
So if its only taking the JMO Manager or Director of Training 6 to 8 seconds to look at your CV and decide your interview fate. Why would you want to risk it on a photograph if you don’t have to? Far better to focus your efforts on making your front page stand out in other better ways as we have written about in the past.
Will the Situation Ever Change?
Probably. And I’m predicting in not too short of a time. A couple of things to look out for here are the fact that the technology for recruitment is advancing into a number of new spaces, including video resumes. Which means that at a certain point a photo on a CV will look more old fashioned than too new. The second thing is that it is now possible through google and social media to relatively easily find a photograph of a person who has applied for a job if you as the recruiter really want to. And in time I would expect that recruitment applications like many other applications become very good at finding the avatar photo that is linked to your email address and automatically incorporate it into your application. Scary huh?
Related Questions
Do I need to worry about having photos on my LinkedIn profiles and other social media profiles?
The Answer to this question is no. How odd does it look when you find a colleague on LinkedIn and they don’t have a picture? Its expected (a social norm) on LinkedIn. As we have discussed above. Its likely that in a not too distant future that we won’t be talking about whether we should be putting photos on CVs. We will be talking about whether we should have a video resume or not.
Are there other things I should avoid putting on my medical CV?
Yes actually. There are several. Chief amongst these is probably unprofessional email addresses. You know the one you made up in highschool on gmail because it was funny. Its always best to strive for a professional sounding email. A gmail is ok if it contains you name and not too many extra numbers and underscores. If you want to up the ante a bit. You can invest in a personal domain name for a few dollars and set up your own branded email address and run this yourself or through Google.
Some other things you should avoid putting on your medical CV are your date of birth (similar reason to the photo) and unrelated hobbies.
What are the important things to have on my medical CV?
For that particular question we have written you an entire post that covers it.
Probably one of the biggest question I get asked by International Doctors is. How do I find doctor jobs in Australia?
In this post, I will try to demystify and break down the process for you. Starting with how to identify suitable posts online and then moving on to other strategies, such as personal approaches to employer and networking.
Now the circumstances do vary a little between if you are working through the standard pathway process, the competent authority pathway process or the specialist pathway process. We will start off by focussing on identifying suitable posts for standard pathway and competent authority pathway doctors and towards the end of the post, I will turn my attention to the specialist pathway.
By the way, if you don’t know what any of these terms mean. Then I suggest you check out the links to them on the Medical Board website OR watch the explainer video below.
Finding jobs. General issues.
There are a number of key steps you need to go through if you are an international doctor or IMG looking for your first post in Australia.
Whether you are coming through the standard pathway or competent authority pathway your first position needs to be one that offers what is termed “provisional registration”. Think of this as a well-supervised post where you get the chance to demonstrate on the job that you are capable of working at the level of an Australian doctor. A year of provisional registration is a general requirement for all doctors coming via either of these two pathways.
Herein lies the problem. Employers in Australia are under no obligation to offer positions for candidates that allow for provisional registration. In fact, by law, they are actually required to prefer Australian doctors over international doctors.
Or to be completely accurate it is a requirement that if an Australian citizen or permanent resident demonstrates suitability for a position that they should be offered that job and it cannot be offered to a candidate from another country.
Okay. But I know international doctors who have gotten jobs here. How does this happen?
Labour markets are subject to issues of supply and demand. And there are often gaps in the supply or number of Australian doctors to fill positions particularly in less popular fields or less popular locations.
So many employers will open the opportunity to international doctors. But usually after trying to recruit an Australian doctor first.
In fact, if you do actually find a position advertised that will accept international doctors it’s quite likely that there will be very few Australian doctor candidates for this position. If any! So that boosts your chances a bit.
“Eligible For Registration”. The Key Magic Words.”
As an IMG looking for doctor jobs in Australia, you can spend a lot of wasted time reviewing position descriptions and ringing potential employers if you don’t know where to look and what to look for.
Think of this as similar to the initial review of a research article that you have found in your search for an evidence-based approach to solving a problem. 9 times out of 10 we will read the abstract of an article (or even just the title) and decide from that that the article is not relevant to our needs.
The same goes for job search and job descriptions. The abstract is the Selection Criteria.
Usually (but not always) these appear towards the bottom of the job ad or position description. Wherever they are find them and look at the criteria. In a doctor job ad, there is always one selection criteria. Normally the first one. That describes what qualifications and registration you need.
The magic phrase you are looking for is “eligible for registration” or words similar to this.
For international doctors looking for a doctor job in Australia. Skip to the selection criteria. The magic words you are looking for are: “eligible for registration.”
Dr Anthony Llewellyn
This means that employers will consider doctor candidates that need their assistance to apply for registration, ie. someone who has their AMC Part 1 or someone who is applying via the competent authority pathway.
On the flip side if you see words like “current registration”, “has registration”, “general registration” or “full registration” this means that you are not eligible to apply for this particular job.
Make sure you check all the selection criteria.
Just because there is a statement implying that the employer will consider someone who is not yet registered does not mean you should go ahead and start putting in your application. You should take care to do a few other things first.
Firstly, you should check through all the other selection criteria. There are normally around 6 to 10 of these. Make sure that you are able to meet all the essential criteria and can give a reasonable impression for any other non-essential (otherwise known as desirable) selection criteria.
Don’t know the difference between essential and desirable criteria? Watch this video.
Next. Go through the rest of the job description. Make sure you understand what the role is about and that you are confident you can at least grow into the role with some help. Pay particular note to where the job is located. If you are not able to commit to working in this particular location. Then don’t apply.
Looking online for doctor jobs in Australia
Looking online is an obvious first place to start if you are looking for your first doctor job in Australia.
The very first thing you should do if you are looking for jobs online is that you should go and register with all the State and Territory Health Department Portals. This is where the bulk of jobs that will be suitable for you are posted. I have put a list of these below to help you out.
You should also register with sites like Seek as most of these systems automatically upload their postings to these general job advertising sites as well in order to increase their reach to prospective candidates.
Most of these recruitment sites have a system of alerts so you can be notified of suitable job openings.
So you should definitely turn these alerts ON.
In most States recruitment is centralized so it’s not necessary to look at each individual hospital or health service.
However, in Victoria, there is a partial centralization through the central system as well as what is called the match system but many jobs are actually only advertised on individual health service sites. So you will need to do a bit more looking around and registering if you are interested in a job in Victoria.
As I said above. The types of jobs you are looking for are ones where they will accept someone who required provisional registration.
The position titles to look at are anything with the word Resident or Resident Medical Officer in the title. These are by far the highest yield job titles. And are the posts that are most likely to be open to International Doctors coming via either the Standard Pathway or Competent Authority pathway.
However, you may occasionally see job titles such as:
Intern
Trainee
Unaccredited Trainee
Senior Resident Medical Officer
OR Even
Registrar
These are either less likely to be advertised (especially intern) or less likely to be open to doctors without registration but are worth reviewing.
In some States. Such as Queensland and Victoria the service will revert to an Award Classification as a title.
So, if you see something like:
House Officer
OR
Junior House Officer
OR
Hospital Medical Officer
That is also worth reviewing.
The key phrase in the selection criteria that you will need to look for is
“ELIGIBLE FOR REGISTRATION”
This indicates that the employer understands that once you are offered the job there will be a process of applying to the Medical Board for registration.
If it just says Must Be Registered with the Medical Board or Have current registration. Then you are not able to apply.
I recommend in order to save time you skip to the Selection Criteria to see if you are suitable.
Trickiness with selection criteria
As a final comment. You will often see additional Selection Criteria requiring certain amounts of or certain types of experience. Sometimes they are happy for that experience to be from anywhere. Sometimes it needs to be from within Australia. Sometimes they may accept experience from one of the Competent Authority countries.
This is becoming a real problem lately and it’s actually pretty poor HR practice.
But it is basically an effort by employers to exclude certain types of candidates either because it cuts down on their workload of interviewing candidates OR because they feel they already have an existing candidate pool with these types of experience.
Some other ways to find a doctor job in Australia
Whilst looking online is going to be your best first starting point. A problem is that it’s also going to be everyone else’s best starting point.
So however clever you think you are at finding those rare jobs that will accept an IMG application you can bet that if you found it then others have as well and have probably shared it with their friends and the dozens of IMG support groups on social media sites like facebook.
The strategies below are easy to implement. They mainly only require an investment of your time.
Its amazing how many IMGs ignore these tactics initially. So, if you want to give yourself an edge over the competition, I suggest you think about implementing one or all of them.
Personal approaches.
Don’t stop at just filling in applications for current vacant positions. Make a list of all the hospitals you are interested in working at and find out who the Managers or Doctors there are who are responsible for entry-level doctor recruitment. Send them a short courteous email with your details and a tailored CV. To avoid it looking spammy try to personalize the email with some sort of information that you have researched about the hospital.
In past roles, I have been added to blind copy (BCC) email lists. It’s pretty obvious when you and a thousand other Medical Administrators have just been sent a CV. I have always trashed these emails. Don’t do this.
I recommend finishing your short email with the statement:
I am interested in any resident level job opportunities that you may have. Or any other suitable positions.
Career Doctor
Don’t try to call at this stage. Don’t be dismayed if you do not get a response. At best you might get a reply to one out of ten emails. If you do get a reply offer to come and meet with the manager or doctor.
Make sure your CV is up to scratch
One reason that you may not get a response is that your CV is not up to scratch. Some of the reasons may be. It contains errors. It might be missing vital information. It may not be well directed to the particular hospital. So before you start emailing brush up on how to write a medical CV in Australia.
Networking.
Networking is not often thought about as an opportunity to identify job positions. But it is. Most international doctors in my experience tend to hang out with other international doctors. This is perfectly ok if you are studying for things like the AMC exam. But it isn’t going to advance your job prospects. Find ways of hanging out with actual real employed Australian doctors. Some examples of how you might do this are by undertaking a clinical observership, going to medical conferences, becoming a medical school tutor, and enrolling in some of the courses that trainee doctors undertake.
There are two key advantages to this. Firstly, you are getting better exposure to what it’s like to work in the Australian medical system. Secondly, as you develop friendships with employed doctors you will start to find out about potential job opportunities as well as get assistance with personal referrals to people in the hospital who are in charge of doctor recruitment. This will help you get through the first filter and have a chance to put your case forward.
Private hospitals.
Most general practitioners are employed in the private sector. So that’s where you need to look if you are after a general practice job. And most general practice doctors have understood this for quite some time.
Private hospitals on the other hand have been a bit overlooked in terms of possible positions for international doctors. This is probably because traditionally to work in a private hospital you needed to be an actual Consultant, a Fellow of a College, who can bring patients into the private hospital and allow the private hospital to charge. Or a fairly senior and experienced doctor who can work efficiently for the hospital and particularly free up the Consultants.
Of late things have been changing. There have been some private hospitals that have started to take medical graduates as part of the intern allocation process. And some hospitals are now seeing IMGs as possible options for providing general ward cover.
You might try approaching these private hospitals individually or many work as part of a group of hospitals where you can apply for a range of job opportunities.
Getting out there.
In my “5 Tips for Working as a Doctor in Australia” video I point out the medical job labor market in Australia is driven by an issue of supply and demand, whereby prestigious hospitals in capital cities are generally sought out by doctors. This means that the cities tend to draw doctors from the regions and the regions from the rural and remote areas.
As a result. The more prepared you are to get out past the big places like Sydney, Melbourne, and Brisbane. And even bypass the Newcastles and Geelongs. In favour of the Burnies, the Rockhamptons, and the Armidales. The more likely you are to be able to actually meet with someone who might be interested in seeing if you are a good fit to work at their hospital.
I speak to so many International Doctors about this tip. And so many ignore this really sound piece of advice. It can be hard to move your family if you are established within a like community in a capital city. But you will often find that there is a lot of local support and gratitude that makes it worthwhile at the other end.
Should I register with a recruitment agent?
In the above video, I talk about the potential benefits of working with a recruitment agency. Sometimes the agencies know about other job opportunities that are not well advertised publicly.
However, it’s not as simple as just registering. Recruitment companies have to make a living. So they are not going to take on any doctor for whom they feel that there is not a real prospect of landing a job.
In my experience, you are wasting your time contacting recruitment agents if you are on the standard pathway unless you perhaps have a prospect of working in general practice.
On the other hand, it may be worth contacting a recruitment agent if you are eligible under the competent authority or have already gone through the specialist assessment process. Particularly if you work in one of the higher-demand areas, such as critical care, psychiatry, or general medicine.
I’m a General Practitioner. How do I find a job?
This is a great question. And, I’m hoping to provide some more information about this for you shortly. Many of the strategies discuss above will work if you are looking for general practice roles. You are not, however, generally looking for those keywords of “eligible for registration.” And you are unlikely to find many general practice positions advertised on the State and Territory recruitment sites.
I’m a Specialist. How do I find a job?
This is a great question. And, I’m hoping to provide some more information about this for you shortly. Many of the strategies discussed above will work if you are looking for specialist positions. You are not, however, generally looking for those keywords of “eligible for registration.”
This month around Australia the new medical graduates join the health care system as Interns. #tipsfornewdocs is an initiative to extend a welcome from #olddocs to the system
Welcome to all those new Interns who have started in the Australian health care system this January.
In the spirit of welcoming you and being helpful we would like you to have a helpful term changeover checklist on us (courtesy of our community manager Rachel.
Its an initiative to connect #newdocs with #olddocs and welcome them to the system and profession. As you can see from our collection of favourite tips. Its now an international phenomenon.