Come back regularly as we endeavour to give you the most comprehensive information on the doctor job application process. All things medical job-related.
Interviewing for a job as a doctor can be stressful, especially when its been a while since you may have had some practice.
A way that some doctors choose to improve their interview skills is to work with a coach. During interview coaching, a doctor meets with a professional coach to learn strategies for being more relaxed about the interview process and of course to perform better.
Should you work with an interview coach? And if so, how can you find a doctor interview coach in Brisbane?
Why Interview Coaching?
The most obvious reason is that interview coaching can help increase your chances of getting a job. There are a number of ways this can occur.
Coaching can help you overcome any nerves or anxiety you have about the process. Coaching gives you a chance to experience answering many different interview questions. Coaches provide you with feedback to help improve your responses during interviews.The more you practice with a coach, the more confident you will become. By engaging with a coach you are also ensuring that you commit to your own practice regimen, which is important for a good performance.
Some reasons you may want to consider engaging a doctor interview coach:
It’s been awhile. If it’s been a few years since the last time you interviewed for a doctor job or if your last interview was fairly simple and you anticipate this one will not be the same, then a coach can help you rehearse and regain your interview confidence.
You get nervous before interviews. A little bit of anxiety is good going into an interview. But too much anxiety can affect performance. Practicing with a coach can help you feel more comfortable, relaxed and prepared.
You get interviews, but not offers. Often its difficult to get honest feedback from medical interviews. A coach may be able to help work out what is going wrong for you.
You are not sure about something on your CV. Maybe you have had to have a break in work. Or your last job didn’t go so well. Are you perhaps switching specialties. A coach can help you with how to tell the right story in relation to these sorts of issues.
Its your dream job and you want to land it. A coach can help with feeling confident in these situations.
On the other hand, if you’re a confident interviewer and have always tended to perform well during interviews, then a coach may not be necessary.
Types of Interview Coaching
There are many types of interview coaching. Some coaches meet with you in person, and others speak with you online or on the phone.In general interview coaches work on something called “performance coaching”. Think of it like a sports coach working with an elite athlete. A key element is practice with feedback. The more practice and the more immediate the feedback the better.
If you meet the coach in person or online, they can also help you develop effective visual communication. The coach can work with you on facial and body expressions that convey trust and show active listening.
Coaches may also help you with other elements of the interview, including how to ask the right questions of the employer, how to research the job and the panel and even some advice on how to dress.
How to Find a Doctor Interview Coach in Brisbane
There are lots of coaches available to choose from in a capital city like Brisbane. Career coaches often offer interview coaching. Some things you should consider in a coach are the following:
What is their training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process. Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Do they provide face to face coaching or on the phone or online. Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session. Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
I wrote this post as I have been collecting questions that are typically asked at a resident medical officer (RMO) interview. So these top 16 resident medical officer interview questions are based upon what job candidates have reported are the common types of interview questions being asked by hospitals in Australia for resident medical officer jobs or what are sometimes referred to as junior house officer or hospital medical officer jobs in Australia.
For resident medical officer interviews, you will commonly have around 20 minutes with a small panel of 3 or 4 and be given between 4 to 6 questions to answer briefly. These will generally consist of:
an opening question about your experience or interest in the role;
questions about past examples of handling conflict or dealing with errors;
questions about strengths and weaknesses; and
at least one clinical scenario where the focus will invariably be on recognising a sick or unwell patient and asking for help early.
So typically these jobs are at a postgraduate year 2 level. Hospitals often post these openings throughout the year in an attempt to fill gaps in their trainee doctor rosters. So these jobs offer opportunities for Australian doctors to move hospitals but also provide opportunities to get their first job experience in Australia.
I am posting this information as it may help both local as well as international medical graduates who are fortunate enough to be offered an interview for a resident medical officer-level job.
The Top 16 Resident Medical Officer Interview Questions.
Question 1. Tell us about your experience and how it makes you a suitable candidate?
I’ve written in another post about how this question is often just asked in the shortened version. “Tell us about your experience.” In which case it’s a very lazy question. It’s often asked because sadly on some resident medical officer interview panels, the panellists are slotted in the day before and do not have time to review your application and CV.
Regardless of how the question is asked you should answer it by telling the panel about how your experience makes you a good candidate.
Do this by picking out one, two, or three of the selection criteria and relating your experience to them.
So, for example, a common selection criterion is communication skills. So talk about how your recent experience has been working in a hospital with lots of patients who are from a Non-English speaking background and how you have had to collaborate (probably another selection criteria) with other members of the team to meet this challenge.
I recommend that you take a portfolio of relevant files to the interview. One of which should be a printout of the selection criteria. This is very handy for working out why they are asking certain resident medical officer interview questions.
Question 2. What are your long term career goals and why this hospital?
This is the other common opening question when it comes to resident medical officer interview questions.
If you have written a Career Goal Statement that is tailored to the job description then you pretty much have the basis of the answer to this question.
This question is digging into whether you have done your appropriate research. Have you identified a reason why the hospital will help you in your career? For example, does it have good exam pass rates? Or is there a particular subspecialty that is not available elsewhere?
Whatever the case you should be able to identify something of value in the position that will help you. Make sure that you are emphasizing that it’s a positive factor about the health service or hospital. Interview panels want to hear nice praise about their institution. But also make sure that you quickly bring it back from your personal needs to what you can give to the hospital.
This should be something or somethings reasonably unique to you and not what other candidates might also choose to talk about. See below for strengths and weaknesses.
Question 3. A member of the nursing staff complains that an intern is not attending calls and not doing duties properly, what will you do?
A big tip for this question is to avoid the inclination to stereotype nursing staff and refer to the nurse in this scenario as female.
Hypothetical scenarios are common in doctor interviews and especially for resident medical officer interview questions. This particular interview question bundles both the potential for work conflict (between yourself and the nurse, yourself and your colleague, and the nurse and your colleague) along with the topical matter of trainee doctor well being and what’s called the trainee in difficulty.
So the key here is to cover all the key principles in the scenario. To show you have a broad awareness of what might be going on.
Another very good tip for this question as well as most other questions is to list your key points first. That way the panel knows what you are thinking, even if you run out of time to address all the issues.
The key points here would be:
How you engage in the initial discussion with the member of nursing staff in a respectful and listening manner.
What your strategy for approaching your colleague is. And again, how you are going to conduct that initial conversation, which is often referred to as a “quiet chat”.
The potential outcomes of your “investigation” into the problem. In particular, how you would handle it if your colleague was resistant and how you would handle it if they confided in you a problem.
Your responsibility to discuss things with more senior colleagues.
Question 4. Describe an error you made in your practice and what you did to fix it?
This is an example of what is called a Past Behavioural Question. Panels like to ask for examples of past work that fit the current job challenges as demonstrating what you do is far more powerful and predictive than saying what you would do.
When preparing for resident medical officer interview questions you should definitely have an example of an error ready to give. As well as one about work conflict (see below).
The key here is to be able to give an example of an error that was significant but for which there was not a really terrible outcome. The best examples are system errors or simple communication errors. If possible it should be something where you caught the error yourself and then there was an attempt to look at the system to improve it for next time.
So for example an error where the wrong data was entered on a discharge summary because the electronic record system was unclear would be a good one. So long as the patient was okay in the end.
Answer all example-type questions using the STAR method.
STAR stands for
Situation
Task
Action
Result
Please. Please. Please don’t forget to give the panel the result of the example. So many times job candidates tell the story but then fail to sell it by going over the results of their actions. If you don’t talk about the results of your actions the panel will assume you are not results-oriented and probably also take feedback poorly. Not good.
Question 5. What strengths do you bring to this role?
This is sometimes answered alongside a request for weaknesses (see also below). If also asked for weaknesses. Start with weaknesses first and give just one. Then end with two or three strengths.
For strengths. Try to come up with something reasonably unique and remember it needs to be relevant to the role.
So things that are not unique to say are:
“I’m an excellent communicator”
“I’m a team player”
Because pretty much everyone does say that about themselves at these interviews.
It doesn’t have to be overly specific. Just something which you can back up. So for example, if you have done a lot of teaching in your career and have good feedback on this. This would be a good strength to highlight in terms of any teaching responsibilities of the role. There are always at least some medical students floating around that need looking after.
Question 6. A nurse is insisting to give medication to a patient whom you don’t know and you don’t know the medication. What do you do?
Some questions seem simple on the surface. But providing a simple answer is not going to get you very far. It’s obvious with this hypothetical question that you should of course not go ahead and prescribe the medication.
But you need to show your awareness of the needs of others in this situation, in particular the member of nursing staff and the patient.
How are you going to discuss your dilemma with the nurse and possible the patient?
Is the situation urgent? Will you need to call your senior for advice?
Do you have time to go away and look up the medication and review the patient’s file?
What will you be telling the nurse? Their job is probably being held up by your current lack of knowledge. So you should be indicating to them when you will be able to get back to them.
For hypothetical scenarios, the CanMEDS Framework from the RCPSC is a great model. It gives you lots of ideas about what sorts of issues to cover. It’s also the framework upon which every Australian medical specialty college has built its frameworks upon.
CanMEDS Framework
Question 7. Describe a situation where you displayed leadership skills.
Again. We are looking for an example here. So using the STAR method is recommended. It’s sometimes difficult as a trainee doctor to find opportunities to demonstrate successful leadership. So don’t forget “followership”. This is where you act like the first person to follow a leader and help them to enact a change.
Good examples are things like noticing a safety or quality problem on the ward and instigating a change. For example, perhaps a ward trolley was inadequately stocked and you worked to improve the situation. Be prepared however to demonstrate evidence of lasting change. Did you go back and check that ward trolley after you left that rotation?
Question 8. What is the importance of documentation as a doctor?
This question tests your awareness of some of the key requirements of the role of trainee doctors. Particularly the most junior trainee doctors where documenting (or dealing with computer information systems) can be 80% of the job on a daily basis!
Obviously documenting IS important. But Why? Again, the CanMEDS framework may be a helpful construct for you in this question.
You might also legitimately answer this question by saying: “Documentation as a doctor is tremendously important and I am going to give you 3 examples of why?” Then give three good examples.
There are so many angles to this question that giving 3 good examples is going to be just as good as covering every point that you could imagine.
Question 9. Describe a situation where there was conflict between yourself and another member of a team?
This question is a big but avoidable trap. You can avoid it by being prepared for it and having an example. Again. The STAR method is your friend and the key here is to be able to demonstrate that you managed the conflict to a point where you were at least able to have a good ongoing working relationship with your colleague.
It is important to not only describe the situation and the conflict. But also take the panel through the steps you took in terms of your communication and collaboration to work with your colleague on the conflict and how you showed respect to them.
Question 10. You are covering the obstetrics and gynaecology wards one evening and a 35 year old female patient who had a caesarian section 2 days ago is now presenting with severe shortness of breath and chest pain. What is your approach?
You can insert here any typical clinical scenario which might happen on the ward where the resident medical officer is called to review. Chest pain and other types of escalating pain are favorite scenarios. Usually, the scenario is in two parts. The initial question is in the form of the information you might be given when a member of the nursing staff calls you.
The next bit is the examination findings. Generally, the examination findings are either of a patient who is deteriorating or already in need of an emergency response.
So the key aspects of responding to these questions are not to give a textbook answer to the clinical problem. But to frame it in terms of your role as a very junior member of staff. You need to spell it out to the panel. You need to let them know that:
You would prioritise the call – Go Straight Away.
You would ask for vital signs over the phone.
You would ask the nurse to call an emergency response. If the vitals warranted it.
You would ask the nurse to stay with you to help.
You would have in the back of your mind a question about “What could be the worst case scenario here?” for example a pulmonary embolus.
You would take a quick history and examine the patient.
You would have a low threshold for calling a senior colleague and/or an emergency response.
Question 11. Describe a situation where you displayed effective communication skills.
This is similar to the conflict question above. And in fact. It is perfectly okay to use the same example to answer more than one question.
Other typical situations to think about for this question, include complex patients and/or patients and families with communication challenges and/or patients and families who are upset with their care.
Question 12. What qualities should a resident medical officer posses? Which ones do you have and which ones do you lack?
This is basically a variation of the strengths and weaknesses question.
But there is also a big hint stating you in the face. The position description, in particular the role statement and the selection criteria. So you can use these to your advantage.
You might start by saying something like:
“Well, I understand from reading the position description that the key roles and capabilities are as such…”
This shows you have done your research and you are willing to align your opinions with the panels’ views of what a good resident medical officer is.
You can then go on to highlight the sort of qualities that an individual might need to meet these criteria and match them to your own.
So for example. The ability to work under pressure is often a selection criterion. So you could talk about this requires the quality of being calm in a crisis and being able to juggle a number of tasks.
How To Talk About Your Weaknesses.
Basically, you should not choose to talk about something that is a big weakness that you have chosen to do nothing about.
You should also not choose the weakness that everyone picks. e.g. “I’m a perfectionist” or “I can work too hard.”
Ideally, you should pick something that you have identified that you are not so strong and have been working on.
For example, maybe you struggle with reading. And you know that this is important for the exams. So you have joined a study group where other members are better readers and you are challenging yourself and keeping yourself accountable that way.
Question 13. Describe a situation where you displayed teamwork.
Again. We are starting to repeat ourselves with this question and questions about communication, conflict, and leadership.
Great examples here are situations where you noticed your colleague was struggling. Perhaps they had a bigger caseload than you. And you stepped in. Others might include helping to onboard a new doctor to the team.
Question 14. You are called by nursing staff and are told that some antibiotics were given to a patient that were actually supposed to be given for another patient, what do you do?
Once again the CanMEDS Framework will be helpful here.
Let’s look at it in more detail.
Health Advocate.
So. Obviously your first concern is for the safety of the patient who was given the wrong antibiotics. Are they allergic? Do they need monitoring? Also, has anyone else been given the wrong medications and needs to be checked?
After this, there is the issue of disclosing to patients and their families what has happened. You are representing the hospital so you need to be able to talk about how you would carry this function out. You need to do the initial disclosure but then be aware that more senior staff should be informed and take it from there.
Communication.
So. There is how you communicate with the patients and families about what has happened. There’s also communication with your nursing colleague and there is communicating with seniors.
Collaborator.
You are needing to work collaboratively with the nursing team to identify all the current risks and deal with them. You also need to be mindful of keeping good relationships with the nursing staff. The nurse may be in trouble for what has happened OR possibly they were doing the right thing and a doctor has made an error.
Professional.
There will be hospital policies and protocols that need to be followed. You may not be aware of all of these but it’s your responsibility to find out about them. The incident will need to be reported and you should be making careful notes of your involvement in case there is an investigation.
Potentially in this scenario, there has been a breach of professional standards. But that’s not immediately evident.
Leader and Scholar.
Is this the only time this problem has occurred? Was it predictable in hindsight? Does there need to be some thought to changes that would prevent it from happening next time or an audit of processes?
You noticed I didn’t even mention a medical expert in all of this.
Question 15. Describe a situation where your consultant noticed that you have made a mistake and how did you react?
This one may be hard for international medical graduates to answer if they have not had any medical work experience for a while. If so, panels will usually accept a suitable example from another job.
This question is a variation of the error question. So again. The idea here is to not produce an example of something where it all went terribly wrong. If you think about it there are probably lots of times where your senior colleagues have pointed things out to you that have helped you improve. We learn a lot from mistakes. And this should be part of your answer.
An ideal answer would include how you encouraged your consultant to give you specific feedback about your mistake so you could improve for next time. Bearing in mind that most doctors are terrible at giving feedback to other doctors. And then how you measured your success.
Question 16. You are the Resident in Emergency and a patient suddenly collapses. What do you do?
Basically another clinical scenario where you are the first responder. You should not forget that even though you are in the Emergency Department you need to call an emergency so that others respond.
Once you start getting into going through the DRABCs. There will probably be some supplementary information provided about the patient. Along the lines of them being in shock. Again. Call for help whilst dealing with this situation.
Bear in mind that it’s a rule that doctors in prevocational roles should not be the only doctor in the Emergency Department so there should be someone more senior to call upon.
Related Questions.
Question: Should I Ask A Question At The End?
Answer. In most cases, you have probably already had a chance to ask questions before the interview. So it’s perfectly fine to say no. But remember that the final question at the end is a chance for you to go back and review some of your answers or clarify anything you feel you may have gotten wrong in the interview.
If you are after a good sort of question to ask. Think about asking for some feedback on how your interview went. Whilst the panel obviously can’t tell you whether you were successful or not. They may have useful insight for you. And this may be your only opportunity to get meaningful feedback.
You might also consider asking the panel what they feel that their biggest challenge is at the moment. Only do this however if you think you might be able to offer some assistance in meeting this challenge.
One of the questions I am most asked by doctors from other countries is: “What is the pay like for doctor’s in Australia?”
We are approaching the period here in Australia where we introduce a large number of graduated doctors to the Australian health care system as Interns.
So at AdvanceMed we thought that we would review what the rates of pay are for Interns in Australia. The findings are quite interesting.
The results above reveal that there is a wide variation of over $10,000 per annum in an intern salary from NSW, which pays the lowest at $67,950 to Western Australia which pays the best at $78,479 per annum.
The reason for the large variation is that each State and Territory sets its wages for public employees separately through something called an Award or an Agreement. These are formal documents that state the conditions of employment. They include matters such as the hours of work, the leave available and of course how much you get paid.
Doctors like other public employees do not generally contract as individuals for their services with hospitals. So everyone gets the same conditions.
According to the Australian Bureau of Statistics Full Time Adult Average Annual Ordinary Earnings is was $82,752 in 2018. So bearing in mind that it takes a minimum of 5 years of university study (with a fair collection of higher education debt to pay off) to get to this point we can certainly not consider Interns to be extremely well paid.
But its not all that doom and gloom. Whilst, Interns certainly do not work the amount of overtime they used to 10 or 20 years ago. Overtime provisions, as well as loadings (working rostered hours on an evening, night or weekend) under most Awards and Agreement can lift the annual take home pay of an Intern significantly. For e.g. most overtime starts off being paid at 150% and rapidly goes to 200%. So, if an Intern works on average 50-60 hours per week they are likely to hit Full Time Adult Average Annual Ordinary Earnings, even in a State such as NSW.
It Goes Up From Here
And, of course it does improve significantly from this position. By the time a doctor becomes a Registrar in Victoria for example, their regular pay has increased to $105,000 per annum (after a period of 2 or 3 years). And a first year Staff Specialist in NSW can earn upwards from $234,566 per annum.
A Special Bonus For Interns
An additional bonus for Interns comes the first tax time. In Australia the Financial Tax Year runs July to June. So, because you have not been paying much in the way of taxes for the first half of the financial year, you end up paying more tax than you need to in your first 6 months of Internship and can get a reasonable return come tax time. For this reason, some Interns seek to work extra overtime before 30th June.
What’s Going On in NSW?
When I was an Intern, NSW paid some of the best salaries for trainee doctors in the country. States like Western Australia (which is now first) were actually towards the bottom of the list.
Given that NSW is the biggest State by population, one of the richest States economically. And given that Sydney (NSW’s capital city) is probably the least affordable place in Australia to live it makes little sense that NSW Interns get paid the least.
Its hard to know exactly why this situation has occurred. Its possible that the industrial groups that represent doctors in other States and Territories have been more successful in representing trainee doctors over the years.
This certainly seems to be the case if one looks at the Enterprise Agreement for doctors in Victoria. Which even includes an allowance for continuing medical education, as well as separate provisions for internal training leave, examination leave and conference leave.
This situation puts the NSW trainee doctors Award to shame. This instrument has not been modified in any significant way since the 1990s (possibly longer).
As we enter the new academic year for medicine in Australia and New Zealand many doctors are thinking about whether they might be applying for a new position in 2020.
Yes. It’s that competitive in some situations. That even before you have commenced your current job you are thinking about the next.
One thing that is vital to ensuring you progress smoothly through the job application process and gain an interview is a powerful CV or resume. We have written about this already here and here and here.
You might even be considering getting some expert assistance with developing your CV.
But before you do. Consider whether it’s not worth the effort to construct this vital document yourself and get it checked or reviewed rather than handing over the entire enterprise to another party.
Why have your CV reviewed rather than engage a professional CV writer?
There are a number of reasons why a CV review might be the better option for you.
Firstly, you can probably find someone with expertise in your own hospital who is happy to review your CV for free. Barring that a professional CV review is a much more affordable option if you want to go down the paid route. (Around $100 for a review versus $300-$500 and more for a CV writing service).
Secondly, by constructing your CV yourself you get a deeper understanding about your own career. Including your strengths, capabilities, weaknesses and what value you can bring to future employers. This is all useful stuff when it comes to the interview.
Thirdly, when you engage a professional CV writer you still have to provide the content and this can be quite a lengthy process where you may feel like you end up writing most of the CV yourself anyways.
Starting a new job in Medicine can be exciting, but it can also be very stressful. How often have you started a new rotation or a new job and felt a bit lost on the first day? Have you ever had an experience where you can honestly say that you “hit the ground running?” Assigning a workplace buddy can help ease the transition for new employees into their new roles can be very beneficial for all involved, especially during the onboarding process.
What is a Buddy System?
Buddy systems have been used in other industries and schools for many years and proven to be effective ways of ensuring that employees get off to a good start. This has all sorts of benefits to both employee and the organisation.
Simply put a buddy system involves assigning a new employee a workplace buddy. The buddy is an existing doctor who guides the new doctor through the first few weeks or months on the job. In Australia we have started to see the rise (or in some cases rebirth) of buddy programs, sometimes also referred to as mentor programs. In particular it is now common in the State of NSW, for the second of the 2 weeks of Intern induction to consist of a “buddy week”, where the new intern gets the chance to understudy a finishing intern in their first new rotation. Whilst these buddy weeks are quite popular they do have their limitations. The key one being that because the relationship is very brief it only really permits a small transfer of knowledge and in particular doesn’t afford the new intern doctor a chance to reflect and ask questions of their buddy about the hidden curriculum of the workplace.
Evidence has emerged that longer relationships between new employees and existing employees in Medicine can help reduce stress, and improve morale, sense of support and job satisfaction.
Buddy systems should include a formal documented process that outlines the buddies’ responsibilities as well as what items they should cover over the first few weeks or months of employment. The buddy system should also encourage the new employee to share tips, tools, knowledge, and techniques they have learned about the workplace. A buddy also potentially gives the new doctor a psychologically safe opportunity to offer confidential feedback about how their onboarding process is going. For these reasons the closer the buddy is to the new doctor in terms of peer relations the better.
Why Implement a Buddy System?
The last thing we should hear from a doctor on their first day is “Nobody knew I was starting today.” At the end of their first few weeks in the job we want new interns to feel that they made the right decision to study medicine and for other doctors starting new jobs we want them to feel that they accepted the right position.
First impressions are key. The initial enthusiasm that interns experience to have “finally made it” can be either lifted or ruined, depending on their start. What happens during the first few days can determine the long-term perception of the job and the organization. Studies have shown that a large number of employees quite within 6 months of taking up a job. Often citing a poor onboarding process or lack of clarification about their role as the key reason for doing so.
Regardless of whether there is a formal process in place or not, onboarding is going to happen; the real issue is the quality of the experience. When onboarding is done well it sets up new doctors for long-term success. If an orientation consists of handing the new intern a pile of forms to fill out on their first day, then there are going to be future problems, which is where a buddy system may come in handy.
Implementing a buddy system can be part of an effective onboarding program that provides new doctors with a way of resolving questions regarding work processes. Some of which may be difficult to predict and / or hard to deal with in a formal orientation seminar. This socialization and support can make a big difference.
In particular, a buddy can help with the last 3 of the 4 C’s of onboarding: Compliance, Clarification, Culture and Connection.
The buddy system is not only valuable to the new doctor. Its obviously also an opportunity for existing doctors to develop skills as a mentor and may foster the early development of a range of people management and leadership skills.
From a bottom line point of view a well executed buddy system will likely reduce the number of doctors leaving a hospital or organisation, particularly early. And this will save the hospital a lot of money in re-recruitment costs.
But at a deeper level buddy systems can improve employee engagement with the organisation which can be a vital component of instilling a positive workplace culture. Which in itself is likely to lead to better outcomes in terms of both patient care and cost.
Benefits To Buddy
Benefits To New Doctor
Recognition
One-on-one assistance and single point of comfortable contact
Expand Network
Jump start on networking
Opportunity To Lead
Smoother acclimation
Fresh Perspective
Knowledge of “how things really get done”
What Is a Buddy?
A buddy is someone who partners with a new doctor during their first few months of employment. He or she is a colleague assigned to assist the new doctor to get through this period. They can provide insight into the daily activities of the hospital and help the new doctor fit in more quickly.
An effective buddy is a good communicator, has an interest in the development of others and is the type of doctor the organisation hopes to emulate (fits with the value system). They will generally take the new doctor around their hospital and orientate them and introduce them to key people who can help them out.
A Good Buddy
Is known as a good performer and well regarded;
Is willing and able to mentor others;
Has the time to be available;
Knows the new doctors job;
Is a peer of the new doctor;
Has good communications and interpersonal skills.
A good buddy should be a good representative for the culture and values of the hospital and organisation and be familiar enough with the formal and informal organizational structures to be a reliable source of information.
Buddies Should Not Be
A buddy is definitely not a supervisor and probably should not be a mentor (at least in the first few months). This helps to make the task of the buddy more limited and definable. Learning how to be an effective buddy can be useful as a foundation step to learning how to be a mentor or supervisor. The buddy is are available to answer straightforward questions about how the hospital operates. It is important to make clear to both the new doctor and the buddy that the buddy is not being asked to develop the new doctor and is not accountable for performance. This makes the buddies role easier in terms of being able to support the new doctor without fear of reprisal.
If a doctor does not want this extra responsibility, then they should not be assigned the buddy role. Some doctors simply don’t want the responsibility or are not ready. Worse, some doctors are not well suited temperamentally for the role. A doctor who is known to be someone who gossips at work is probably not a good fit for a buddy role. The last thing a new doctor wants to hear about is gossip and speculation in their first few weeks.
What Do Buddies Do? What Training and Support Do They Need?
Buddies should be given the skills and knowledge to be able to:
Teach or tutor, for e.g. explain an unfamiliar task;
Explain tactical matters, such as how to submit a time-sheet and where the pathology forms go;
Talk about and explain the hospital’s structure, written as well as unwritten rules;
Share insights on how things are done in the hospital;
Involving the new doctor in social activities, such as coffee and lunch with new team.
Buddies can benefit from some training and support in their role. But probably the best thing that can be provided is a suggested list of task and a timeline for completing them.
Generally speaking the buddy is encouraged to meet more frequently with the new doctor e.g. daily for the first week, weekly for the first month, monthly for the next few months and gracefully exit from the relationship. Its helpful to set a solid time frame for when the relationship finishes (6-months is generally good).
During the first few meetings the buddy works to help with urgent and practical questions. As the relationship matures and the new doctor finds their feet the explaining turns into more of the “why things are done this way around here.”
Tips for Being a Buddy
If you are asked to be a buddy, here are some tips that can help you:
Keep a list and timetable of what things the new doctor needs to know or be shown;
Be patient. Relationships take time to develop. Your new colleague is unlikely to open up to you until they have spent a bit of time getting to know you and you have earnt their trust;
You are not the expert on everything, instead think about who else can answer questions you don’t know the answer to and introduce them to the new doctor;
Don’t try to cover everything at once. Remember the new doctor is going to feel overwhelmed in the first few weeks. So try to avoid cognitive overload. Leave the deeper discussion till later;
Stay positive. New doctors will grow into their roles in time with appropriate support and confidence is infectious. Maintain a positive, teaching attitude;
If possible try to identify the new doctor’s personality and communication style and adapt;
Be open and don’t judge. Your new doctor is relying on you to be a safe place to get answers to their many questions.
Remember. Despite the best efforts of the manager who asked you to be buddy. Sometimes buddy relationships don’t work out. Don’t be afraid to approach your manager to express concern and/or suggest an alternative buddy.
Troubleshooting Problems With Buddy Programs
There are some practical problems with assigning buddies in hospitals. Firstly, there are often not enough experienced buddies to go around. Especially with 100+ new interns starting all at the same time. Secondly, often those who are identified to act as buddies are taking leave or moving on at the same time as when the new doctors are arriving.
One way to get smart about this issue is to gather information and consider the level of readiness of the new doctors. There are likely to be some in this group that require more support than others. Typically some may have already studied as student or worked in the hospital already and have a level of familiarity. These new doctors can probably more safely be assigned less experienced buddies and you can save your best buddies for the completely new doctor.
Setting up regular training and check ins with your buddy group can identify gaps and issues. This can be triangulated with sessions with the new doctors themselves.
Facts
Cognisco in 2008, estimated that UK & US businesses lose $37 billion annually because employees do not fully understand their jobs. According to their white paper, “$37 billion: Counting the Cost of Employee Misunderstanding.”
Summary
Creating a buddy system for new doctors requires some time investment and buddy choice should be carefully considered. However, this is not a difficult or expensive option to implement.
Make sure you’ve chosen a willing and effective buddy; create some documents to support them and the new doctor. Set an end date for the formal buddy relationship. Watch for the things that do not work so you can guide both the experienced and new doctors.
A buddy system can dramatically reduce the time a new doctor requires to be productive and aid retention. An additional benefit of a buddy program is that it allows for corporate knowledge sharing and positive recognition for the buddy.
References:
Cooper, J. & Wight, J. (2014). Implementing a buddy system in the workplace. Paper presented at PMI® Global Congress 2014—North America, Phoenix, AZ. Newtown Square, PA: Project Management Institute.
Some Things You Ought To Consider If You Are Planning On Medical Interview Coaching This Year. Before You Commit
Are you planning on undertaking medical interview coaching in 2019?
A Wrap Up Of 2018
2018 was another successful year for coaching clients. Demonstrating the value of performance coaching to secure career progression. We managed to help clients secure some fairly competitive posts, including Visiting Medical Officer, Managerial roles & Advanced Training roles. As well as gain entry to some prestigious training locations (think Prince Alfred & St George in Sydney & The Alfred in Melbourne).
Overall I’m probably most proud of helping one particular trainee. This was someone who was seeking to return from family leave to complete their advanced training part-time and facing a fairly discriminatory employer environment (despite all the overt signs and signals of EEO and encouraging part-time and job-share arrangements).
This was a reminder to me of some of the poor practices (and attitudes) that still pervade doctor recruitment panels in Australia. I took the time to write about this in a joint post with my colleague Dr Amandeep Hansra.
Earlier in the year I was also fortunate to do a review of medical recruitment practices for the RACP and was made aware of some innovative practices in relation to recruitment, in particular a move towards Multiple Mini Interviews for Trainee Selections. I predict we will see more MMI panels over the years. As well as what I am terming “hybrid MMI” approaches (these are generally interviews with two separate panels).
Whilst the median number of coaching sessions for 2018 was once again 3. Some coachees, in particular trainees, opted for an additional fourth session.
Some also approached me for some “last minute” coaching. A once-off interview coaching session can be challenging. Particularly in relation to not overloading the coachee with too much new information. However, many doctors reported these sessions as helpful, particularly in being able to calm their nerves prior to the interview and to ask background questions and test out potential work examples to use.
There remains no doubt in my mind, however, that a planned and stepped out coaching approach is far superior and will address higher levels of interview capability and performance.
Key Observations
The format of most interviews remains remarkably conservative. Usually a single small panel of 3 to 5 running for 15 to 30 minutes (shorter for more junior roles, longer for more senior)
The types of questions remain highly predictable and if you practice enough you will likely cover the majority (with slight variation) bar any clinical problem they may put to you
Questions about experience (some what of a waste given they already have your CV), conflict resolution, strengths and weaknesses and preparedness for the position remain popular
Ethical questions, particularly in relation to trainee doctor wellbeing and managing upwards appear to becoming more popular
Most doctors can identify 3 or 4 good examples (good stories) from their CVs that can be used to fit the range of interview questions. Sometimes to more than one question and even if an example is not asked for
Thanks to our community and coaching clients. We have now collected more than 420 interview questions. Providing a useful bank of questions for you to practice upon.
Key Considerations For Interview Coaching
Career coaches often offer interview coaching. There are lots of coaches available to choose from if you live in a capital city. Less so in rural and regional places. But video technology now lets you connect virtually and also offers some additional benefits (such as not having to travel and the ability to record sessions easily). Some things you should consider in a coach are the following:
What is the coaches training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process? Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Does the coach provide face to face coaching or on the phone or online? Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session? Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching?
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
My Approach For 2019
I have a passion for medical career development and truly enjoy working with other doctors in a coaching format to reach their goals.
For 2019, I will continue to be offering the 3 session online coaching service as my main format for coaching doctors who wish to improve their medical job interview performance.
As an additional bonus for 2019. Doctors who sign up for 3 sessions will receive a complimentary course of their choice tailored to their needs (e.g. CV, Job Application or Job Interview Skills Course).
All this in addition to the ability to offer coaching at a mutually convenient time in the comfort of your own home (or private work area if you prefer). With a recording of each session available to review usually within the hour.
I am always happy to work with doctors on a once-off basis when I can. But I will continue to prioritise coaching clients on a sessional coaching plan.
With AdvanceMed I managed to secure my first preference for Advanced Training. I was able to work on the confidence of my interview approach and believe I delivered a much better package thanks to the training!
Practice an opening type question, during which we can also introduce some techniques for relaxing into the interview.
Go over your work examples as they relate to particular common questions.
And review some interview answer frameworks.
What Are The Benefits of a Series of Coaching Sessions?
Everything that is covered in a once-off session can be covered but with more depth and the opportunity for deliberate practice so that improved performance sticks and generalises.
We also use the extended time to develop better examples and practice answering multiple questions in relation to past example and hypothetical frameworks.
Over this time you incorporate relaxation and “panel warming” techniques into your answer approach. You become better at selling your examples and competencies and agile at answering a range of questions.
Crafting an effective medical CV or resume is a crucial step for medical professionals in advancing their careers. In this updated guide, we delve into the essentials of creating a CV that stands out, combining our extensive experience with the latest trends in medical recruitment.
One of the interesting aspects of medical training is that we tend to assume that doctors have the professional skills to manage their careers. However, it’s been my experience that many doctors struggle with the job application process because this has not been the focus of their training to date. So if you are feeling a bit lost as to what to write in and how to write a medical CV. Here’s an overview.
How To Write a Medical CV. The Best Way.
The key things to writing a successful medical CV are to:
Understanding that employers spend about 6 or 8 seconds the first time they look at your CV.
The final document that employers actually want is more a resume than a CV.
Pay close attention to what you put on your front page. Everything that is good about you should be on the front page. This includes your basic details, short qualifications, recent work achievements and a summary.
Tailor your CV to the role you are applying for. The best way to do this is provide a Personal Summary or Career Goal Statement as the first block of writing. This way you get to control the initial narrative. Not the reviewer.
Don’t worry too much about page length. A good CV should be as long as it needs to be and no longer.
Don’t put a photograph on your CV. This introduces unnecessary bias.
Do make your name the biggest thing on the front page. That’s what you want them to remember.
What’s The Purpose of a Medical CV or Doctor Resume?
The aim of your CV or Resume should be to present a summary of your career, including education, professional history and job qualifications with a strong emphasis on demonstrating that you have the specific skills related to the position you are applying for.
The person who is shortlisting candidates for interview will on average be spending only a few seconds to review your CV the first time. Their primary aim at this stage is to determine whether your application should be considered further. Therefore, the purpose of knowing how to write a medical CV is to ensure that you develop a CV that moves you forward in the application process. You should ensure that your CV is relevant, clear and concise.
What Exactly Are You Writing? A CV Or A Resume.
Let’s start firstly with defining what this document that you are writing is all about. I’ve seen quite a few blogs and posts about how to write a medical CV or how to construct a medical resume. For example this one. But they all seem to skip a basic issue.
Which is whether you are actually compiling a CV or a Resume? In a funny little typical Australian quirk, most medical employers ask you to submit a CV but in fact they don’t really want a CV. That’s just what they call it.
The Meaning of Curriculum Vitae
Curriculum Vitae means course of life in latin. A proper CV therefore is literally a blow by blow account of everything that has occurred in your career and would stretch into several pages for many doctors.
The Meaning of Resume
A Resume on the other hand comes from the French meaning to interrupt and therefore is meant to be an abridged and tailored account of your career. You are tailoring your career history and achievements to best address the job you are currently applying for.
So in fact what you are really writing is more akin to a resume. But you still need to ensure that certain information is included, in particular all your educational qualifications and history as well as all your work history.
Where To Start With Your Doctor CV.
The CV is bookended by the front page and the referees which come at the very end. These are the two most important elements of a good doctor CV or doctor resume. So when someone asks me how to write a medical CV, the obvious starting point for my explanation is with the front page. We will discuss this in more depth and then move on to the other elements.
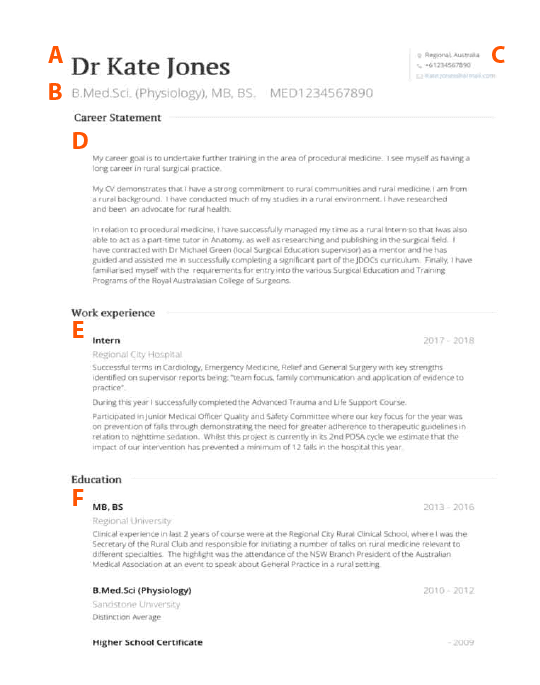
First it may be helpful to illustrate what I am talking about. The letters in the image indicates different parts of your CV.
Diagram: The importance of the front page is illustrated above
A – Your name should be the most prominent item on your CV
B – A qualification summary helps the employer to quickly determine whether you are eligible for the position. It also means you don’t need to put your education history on the front page. Its also a good idea to include your medical registration number. If you are an International Medical Graduate you could also include your english test results and visa status.
C – Provide contact details to make it easier to get in touch. A mobile phone number and a professional email (which you check regularly) are key.
D – A career statement or personal summary is crucial. Think of it as an executive summary where you get to control the narrative of your career.
It should demonstrate why you are a good candidate for the job by drawing on key items in your CV. You should also show how you can add value to the employer. If using a career goal summary format try to set your career horizon 2 to 5 years into the future.
E – Employers are most interested in your work history. This should be written in reverse chronological order. Don’t waste space listing too many details of the position (i.e. specific dates of rotations and job responsibilities) instead use this as an opportunity to highlight your achievements with additional narrative.
F – If you have worked more than 2 or 3 jobs already you probably will not have space for education history on your first page. If you do have space try to ensure you once again make this section relevant to the post and supportive of your career statement.
The Front Page.
The Front Page is where you should focus your effort most. So its best to at least start here. Remember you can always make a draft of this bit then fill in other remaining elements and then come back to it.
Don’t worry too much about formatting for now. Just open a word document and concentrate on the content and the order. Try to keep all your formatting, text and styling to a minimum so that you can do that at the end. That way you will have a more consistent look.
Alternatively, you can use one of the many online CV builders that are available. I recommend VisualCV because it is free to use and if you want to upgrade to one of their slightly nicer templates you can do so for a few dollars.
6 to 8 Seconds To Review Your CV.
Whats all this fuss about the front page? Well, studies show that experienced recruiters spend only a few seconds reviewing your CV (or resume) on the first pass and that most of this time is spent on the first page.
The front page is therefore extremely critical. It should be where you put all your best information. This makes it easy for the person reviewing your CV to determine that you are worthy of a more deeper review. Which in most cases means progressing to the interview phase.
The Front Page should consist of the following elements (see the hot-spotted image):
Your Name – which should be the biggest thing on the page because you want them to remember your name*
Your contact details – you want them to be able to find you
Your short qualifications
A career statement or personal statement
Your work history in reverse chronological order
If you have any space left. Which most doctors do not. You can start to account for your educational history. Again in reverse chronological order.
I’ve written before about the importance of the career statement. But remember this is where you can highlight all the other good things that are worthy of being on your front page. The things that are buried on pages 2, 3, 4, 5 etc… because you are following the rule of work history first, then education history.
Your Name Is The Hero. Not Your Photo.
For an in-depth explanation as to why photos are not recommended on medical resumes go here. The 3 main reasons are that photographs can unnecessarily bias the reviewers impression of you as a candidate, are seen by many panel members as breaking an informal rule AND take up a lot of that valuable 6 to 8 seconds that the reviewer spends reviewing your CV the first time.
What you do want to stand out on the page is your name. This seems an obvious point. But I have seen plenty of CV and resumes where the applicant used a small heading for their name. If you are going to go big with any font and any styling (sometimes a dark background header with your name in white looks good, but don’t go too crazy) then make it your name. You want the reviewer to remember it AND when they go back through that pile of CVs the next time be able to easily find it.
Lots of Narrative Please!
Its important to talk about yourself in your CV. Control the narrative from the start with your career goal statement. But don’t switch straight over to bullet points for the rest of your CV. There are probably some really memorable moments in your work career and education and they deserve a sentence or two if they relate to the job that you are aiming for.
Too often on CVs and Resumes candidates waste valuable space listing all the job specifics (e.g. dates and locations and role responsibilities) whilst not talking about what they achieved or learnt in the role.
Try not to bore the employer.
In most cases you can safely assume that the employer knows what an Intern does on a daily basis. So use the opportunity to talk about the unique things you did as an Intern.
For example, perhaps you are aiming for a specialty trainee position in emergency medicine and one of the selection criteria is about rapid decision making.
Perhaps in your intern or resident role you had an opportunity to demonstrate rapid decision-making? Maybe you worked one doctor down for a significant period so had to bring those skills to bear. If so, write about this element of your work history and relate it to how it will help you in the new role.
“Nailing” Your Personal Summary Section.
Your personal summary section (or Career Goal Summary if you prefer this approach) is arguably the most important section of your CV or resume.
Writing a personal summary for your medical CV is a strategic exercise in controlling your professional narrative. This concise, introductory segment empowers you to set the stage for your entire CV, allowing you to steer the focus towards your most compelling attributes and experiences. It’s an opportunity to succinctly articulate your career objectives, strengths, and unique selling points, framing your profile in the light most favorable to your aspirations.
By carefully crafting your personal summary, you can guide the reader’s perception, ensuring they view your experiences and qualifications through the lens you’ve designed. This deliberate shaping of narrative is particularly important in the medical field, where differentiating oneself in a sea of highly qualified professionals is crucial.
This concise section allows you to highlight your most significant achievements, skills, and experiences, setting the tone for the rest of your CV. It’s particularly beneficial for illustrating how your background aligns with the specific needs of the role and the organization. Moreover, a well-crafted personal summary can differentiate you from other candidates by showcasing your individuality and professional ethos.
The V.E.G. Approach to Personal Summarys.
My favourite mnemonic for aiding in crafting your Personal Summary is the V.E.G. appeoach.
Value in the Personal Summary:
Integrating ‘Value’: You should always lead with the key value you bring to the role. For instance, achievements like implementing a telehealth system or leading health outreach programs can be highlighted to show how you as a candidate can lead and enhance the team.
Ease of Transition:
Highlighting ‘Ease of Transition’: It’s important to allay any fears the panel may have that this job is “too big a step up” for you. Provide examples of how you have mastered key aspects of the new job in your current or previous roles.
Gratitude in the Application Process:
Expressing ‘Gratitude’: Finally it’s important to finish your personal summary by conveying a sense of passion for the role and gratitude for the opportunity. What do you like about the job or the team or the hospital? How will this job help you out? Panels will generally award jobs to candidates they feel will be grateful.
Talk About Your Achievements.
I’m hammering the point here a bit. But it is important to sell yourself. Try to put down at least one important thing that you did in your most recent 2 job roles. If you can back this up with hard statistics. Like “implemented a new pre-admission protocol that reduced the number of patients needing to be re-scheduled for day surgery by 10%” that’s even better.
But maybe its just a compliment your received from a grateful family or something unique your consultant wrote about your performance on your end of term report.
Think also about what things you did that were special in medical school and write about one or two achievements there. Anything that shows leadership or organisation or teaching skills is good. So examples might be being secretary for a club or tutoring pre-clinical students. For the former you can talk about what the aims of the club were and what was achieved that year. For the latter you can talk about how many students you tutored and if you do have some teaching evaluations you can talk about these as well.
The Order. And The Rest.
The expected and recommended order on a Doctor CV is as follows:
Details (name, contacts, registration, short qualifications),
Career Summary,
Work History (Achievements) most recent job first and following in reverse chronological order,
Education History, again most recent qualification first,
The Rest,
Referees.
With “The Rest”. Its totally up to you what you put how you list it and in what order.
If your teaching achievements sell you best then put this next. If its your skills put that next etc…
Some other headings you may wish to consider using are:
Teaching
Professional Development
Publication
Academic Achievements
Extra Qualifications
Qualifcations
Certificates
Volunteer Work
Research
Skills
Publications
Quality Improvement
Leadership and Management
Committees
Presentations
Conferences
Languages
Computer Skills
But again. I emphasis you don’t need to use all of these.
Don’t Worry Too Much About Research If You Haven’t Done Much.
Many trainee doctors fret that they don’t have 10 peer review publications to list on their CV and that this will count badly against them. For most of the jobs that you are applying for research will at best be a secondary consideration. The panel will probably be more worried if they see a CV that has an excessive amount of research listed. As they will get the impression that you may be more interested in research than looking after the patients on your team.
There is no rule that says you have to put the word “Research” as a heading on your CV. You could for example use something else like “Publications” which gives you a bit more breadth to talk about your academic profile. For example maybe you have presented a poster at a conference. That’s a publication. Even blog posts are now becoming recognised as scholarly activities.
You can also focus on related areas such as quality improvement. Perhaps you were involved in an audit as well as teaching (for e.g. grand rounds presentations). There’s lots of scope here.
And as I say. Not having much research rarely counts against a candidate. The only situation that it might count against you is in college selection where sometimes points are awarded for having certain qualifications or amounts of publications.
Referees.
Referees are arguably the most important aspect of your CV. Especially if you make it through to the interview round. Your referees should be contacted to provide some information about you. This information is gold and should be treated as more important than the actual interview itself.
This is the reason why referees are placed last on the CV. It makes them easier to find.
Experienced recruiters know to weight the value of a well taken reference or set of references above the quality of your interview performance. This is because studies show that references have greater predictive validity in selection.
Sadly, many of the doctors you will encounter on selection panels do not know this fact and place too much emphasis on the interview performance. But this does not mean that they are not interested in your referees. They are.
Who should I choose for my referees?
In most industries, your first referee will be your current supervisor or manager and your second referee will generally be you’re the previous supervisor or manager. Medicine is a little different because trainee doctors are rotating around frequently and are interacting with several supervisors and managers on a regular basis.
There are three key principles that I outline to trainee doctors when selecting referees.
The first is recency, the second is relevancy and the third is diversity.
Recruiters will generally want to speak to someone who has recently worked with you, preferably your current manager. In some circumstances this is a requirement. Some good options for this might be your Director of Training, Director of Medical Services or Medical Workforce Unit or JMO Manager.
You also want at least one referee who is relevant to your chosen future career. For most this generally means one Consultant who is a Fellow of the Specialty College you are aiming to enroll with. Some doctors in training try to have 3 College Fellows listed as their only referees and worry if this is not the case. It can be incredibly hard to collect 3 good referees from one College and I actually don’t recommend this approach. You are far better off focusing on obtaining one College referee who has actually supervised you in a term. Most trainee doctors will have a chance to work one term in their preferred specialty before applying for posts.
So who else might you ask to act as a referee?
This is where diversity is a consideration. There may be a Consultant from another specialty who you got on well with in their term. If so, it’s a good idea to put them down. Other options include: Nurse Managers, Senior Allied Health Professionals and Advanced Trainees. The key consideration here is that these should be people that you have worked with who have gotten to know you reasonably well.
I would also recommend that at least one of your referees is male and at least one is female.
By having a diverse list of referees you are telling the selection panel that you value teamwork and the roles of others in the team and also that you are able to get on well with a range of different people in the workplace.
By having a diverse list of referees you are telling the selection panel that you value teamwork and the roles of others in the team and also that you are able to get on well with a range of different people in the workplace.
Anthony Llewellyn
Are there some referees I should avoid or seek out?
As a trainee, you may be worried that a certain referee may be tougher than another referee or that some referees carry more wright because of their name, reputation and connections.
There is really no hard and fast way of knowing whether a referee is more or less likely to improve your chances of an interview or successful job application. Gut feel is probably your best ally here. If you feel that you have established a good authentic working relationship with a referee, they are likely to give you a good reference or at worst a balanced one.
Personally I would avoid any referee that infers that their name on your CV will carry some sort of additional weight.
How many referees do I need?
The short answer is 3. The panel will be required to contact at least 2 referees and they usually only collect 2. The third referee is there in case one of your other 2 referees are not able to be contacted. There is no rule that says you have to stop at 3 referees. You can list more and it may be sensible to add a couple of more referees if you feel that this enhances your candidacy. Extra referees can for example demonstrate your ability to be a team player by listing additional referees from a range of areas of medicine and a range of disciplines.
More than 5 or 6 referees is probably excessive and you should also be mindful of the order in which you list your referees.
How to order and list your referees.
Remember that the first two people listed on your CV as a referee are the ones that will be contacted first for a reference. So you should generally order your list of referees in the order that you would prefer them to be contacted. However, if one of your referees is someone you have not worked with in over 12 months then you should either rethink using them as a reference or put them a bit further down your list (3 or 4 or 5).
e.g. Dr Sandy Duncan, Head of Department of Medicine, St Cliffs Hospital, Sydney
You may wish to add relevant qualifications (e.g. College Fellowship) if this clarifies the nature of the referee better. But you don’t need to list all of their qualifications. You generally do not need to provide a physical address or postal address.
If possible list a mobile phone number and email address as this makes the job of the person taking a reference much easier.
Referees available upon request.
Sometimes you may see the words “Referees available upon request” listed on a CV. This might occur for example when applying for more senior training or consultant posts. It is generally done when you may wish to ensure that you speak to your referees prior to them being contacted by someone from the selection panel, for example where there might be some sensitivity around you leaving your current role
What Is the Optimal Length For a Doctor CV or Resume?
If you look for advice online about Resume length you will quickly be told that a resume should be no more than 2 pages. This is however unrealistic for most doctors. Because we tend to move jobs initially once a year when starting out we tend to accumulate a lengthy work history fairly quickly. Along with this also normally comes publications or extra professional development which is worth including.
The optimum length for a doctor CV or resume should be as long as it needs to be and no more. Practically getting it down to 2 pages is unrealistic. Most doctors can comfortably restrict their CV to a maximum of 4 pages. But again the emphasis is on what information needs to be provided. Not how much. Your emphasis should always be on relevance and creating a narrative that sells you to the employer, so if that means going a little longer in length then that is fine. So long as you spend most of your time refining your front page.
Tips For Ensuring That Your Doctor CV (Resume) Stands Out In A Good Way – How To Write a Professional Medical CV.
As long as it needs to be — Your CV should give the reader enough information for them to explore relevant points during the interview. Most are able to manage this in 4 pages but remember that quality is much more important than quantity.
Do not waste valuable space — Don’t include a cover sheet or index in your CV. Don’t be overly inclusive in relation to specific rotation dates and job duties unless this aids your application.
Easy on the eye — Avoid using too many fonts and lots of different formatting styles (such as bold, underlining, and italics) as this will draw attention away from what matters the most in your CV—the content. Use the same font throughout. A “sans serif” style font, such as Arial is best as these are easier to read. Ensure that the layout, spacing, and structure of your CV are consistent throughout and do not differ from section to section.
Avoid block after block of text — It is better to present your skills and achievements in a given section as bullet points rather than paragraph after paragraph of solid text as this can be off-putting and daunting to the reader. However, this does not mean that you cannot still use a narrative approach. The aim of a good CV is to make your experience and achievements leap off the page.
Do not make things up — Your CV is a statement of fact, and if it is found to include information this can be very bad for your career.
*Never include a photo on your CV. Unless this is mandated.
Related Questions.
What is a Career Goal Statement?
A Career Goal Statement is a summary of you as a candidate. What you are looking for and how you can bring value to the role and the employer. For further details check out this post.
Is there a recommended formula for referees?
For most posts its recommended that you get a mix of referees. At least one referee should have supervised or managed you in the last 6 months. Have at least one consultant from the specialty you are applying for. Try to have a mix of male and female and strongly consider having at least one referee who is outside of the medical profession.
Do I need anything else other than a CV to apply for a job?
The things you will generally also need to put in a job application are a cover letter and you will need to complete a form. Normally this form is online as part of the employer’s erecruitment system. If you have written your CV and cover letter well you probably have all the information you need to fill in the application, including addressing the selection criteria.
How long should my Medical CV be?
Your CV should be as long as it needs be. But no longer. Remember to only including information that is relevant to the job you are applying. For example, if its a clinical role with not much research it’s probably best to shorten up your research section to recent and relevant activities.
Don’t sacrifice page length for aesthetics. If you need an extra page so it looks well set out then use that extra page.
As a basic rule of thumb most RMOs and Registrars will be able to get their CV to 4 pages. Most Advanced Trainees and Consultants might need 6 to 8 pages.
How often should I update my Medical CV?
Short Answer. Each and every time you apply for a new position.
Try to keep a “master CV” somewhere with all your experiences and achievements. LinkedIn can be useful for this.
Review your master CV alongside your most recent CV. Make a copy of this recent CV and update it for the new job adding in relevant components from your master CV.
Can I include volunteer experiences and hobbies on my Medical CV?
Yes you can. But try to show how these are relevant to your ability to perform the job. Some volunteer experiences and hobbies will be more obvious for this than others.
Interviewing for a job as a doctor can be stressful, especially when its been a while since you may have had some practice.
A way that some doctors choose to improve their interview skills is to work with a coach. During interview coaching, a doctor meets with a professional coach to learn strategies for being more relaxed about the interview process and of course to perform better.
Should you work with an interview coach? And if so, how can you find a doctor interview coach in Melbourne?
Why Interview Coaching?
The most obvious reason is that interview coaching can help increase your chances of getting a job. There are a number of ways this can occur.
Coaching can help you overcome any nerves or anxiety you have about the process. Coaching gives you a chance to experience answering many different interview questions. Coaches provide you with feedback to help improve your responses during interviews.The more you practice with a coach, the more confident you will become. By engaging with a coach you are also ensuring that you commit to your own practice regimen, which is important for a good performance.
Some reasons you may want to consider engaging a doctor interview coach in Melbourne
It’s been awhile. If it’s been a few years since the last time you interviewed for a doctor job or if your last interview was fairly simple and you anticipate this one will not be the same, then a coach can help you rehearse and regain your interview confidence.
You get nervous before interviews. A little bit of anxiety is good going into an interview. But too much anxiety can affect performance. Practicing with a coach can help you feel more comfortable, relaxed and prepared.
You get interviews, but not offers. Often its difficult to get honest feedback from medical interviews. A coach may be able to help work out what is going wrong for you.
You are not sure about something on your CV. Maybe you have had to have a break in work. Or your last job didn’t go so well. Are you perhaps switching specialties. A coach can help you with how to tell the right story in relation to these sorts of issues.
Its your dream job and you want to land it. A coach can help with feeling confident in these situations.
On the other hand, if you’re a confident interviewer and have always tended to perform well during interviews, then a coach may not be necessary.
Types of Interview Coaching
There are many types of interview coaching. Some coaches meet with you in person, and others speak with you online or on the phone. In general interview coaches work on something called “performance coaching”. Think of it like a sports coach working with an elite athlete. A key element is practice with feedback. The more practice and the more immediate the feedback the better.
If you meet the coach in person or online, they can also help you develop effective visual communication. The coach can work with you on facial and body expressions that convey trust and show active listening.
Coaches may also help you with other elements of the interview, including how to ask the right questions of the employer, how to research the job and the panel and even some advice on how to dress.
How to Find a Doctor Interview Coach in Melbourne
There are lots of coaches available to choose from in a capital city like Melbourne. Career coaches often offer interview coaching. Some things you should consider in a coach are the following:
What is their training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process. Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Do they provide face to face coaching or on the phone or online. Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session. Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
Coaching
For Job Applications || For Interview Practice || For General Needs
We review some of the official Doctor CV Templates for Australia and New Zealand and give you our findings
As someone who advises a lot of other doctors about medical job applications I am often asked for advice about CV templates.
So I thought that I would review these for you and give you my thoughts.
The key question here is whether it is better to use the template or not?
Overwhelmingly my advice is to not fill in the template. Your CV or Resume (and we really ought to be calling it a Resume because employers do not wish to see the full box and dice) needs to stand out to improve your chances of being progressed to an interview.
So why reduce your chances by submitting a document on an official doctor CV template so that it looks the same as a number of other people applying?
There is an obvious exception. In some circumstances, you are required to use the template. So in this case you should obviously do so.
Notice I am saying “don’t fill in the template”. Which is not the same as not reading it. This brings me to my first key point.
If we look at the majority of these CV templates they are really asking for some pretty basic information which would generally be covered in any typical CV format by an Australian trained doctor. If you took your time to complete your CV properly.
In fact, many of these templates bear a remarkable similarity to the AHPRA template guidelines. Which if we read the purpose of this particular template on the AHPRA website is a “guide to what you should include in the curriculum vitae that you provide to AHPRA as part of your application [for registration]”. This document was particularly written with international health professionals in mind. To ensure that they provide AHPRA with the information it requires to make a determination about registration.
Note here that the AHPRA template refers to being a guide and the MINIMUM amount of information required, which many of the other Australian State CV templates do as well, including Western Australia, Tasmania, Queensland and South Australia. NSW Health does not have a template. I could not find one for the ACT or the Northern Territory. Only Victoria has a compulsory CV template, with various variations for different jobs using the PMCV match system.
In New Zealand, the ACE RMO template (the one you fill in to apply for an intern position) is also a guide. I did find that the Auckland Doctors recruitment site (which would possibly be the biggest recruitment group for trainee doctors in New Zealand) does have a compulsory template.
An interesting observation is that very few of these templates suggest or request a photo, which I am not a fan of. Even in Victoria, where the intern template is compulsory, the inclusion of a photo was voluntary in 2018.
So by all means read what is required, ensure that what you write clearly covers this (I suggest using the same headings where possible) but don’t feel you need to stick to the actual template.
Which brings me to my final observation.
With the exception of the Queensland Health template (which gets a notable mention), all of these templates are quite ugly. You can do far better in terms of a well set out, easy to read and aesthetically appealing CV or Resume.
It’s the start of 2019 and a chance to think about your plans for your medical career this year. Here are a few tips to get you started. Along with a doctor CV example to show how to put these tips into practice.
1. Tidy Up Your LinkedIn And Other Social Media
LinkedIn is becoming a must-have for professionals and doctors are no exception. Not only is it a great platform for storing your education, work history and past achievements. It’s also a platform for getting noticed. So you don’t want future and prospective employers to be reviewing your LinkedIn profile and noticing something awry. There’s nothing worse than checking out a LinkedIn profile where the candidate’s last position is listed as Intern at Hospital X, when they are now a Consultant. Make sure everything is up to date.
Whilst you are at it. Make sure you go through facebook and twitter if you use these. Facebook is now also a platform where some are establishing a professional profile. So if that’s you, make sure everything is professional to public viewers AND/OR review your privacy settings.
Go through your Twitter feed. Think about deleting any Twitter posts (as well as retweets) that may be seen as controversial by any employer.
2. Reconnect With Your Referees
It may be some time since you have spoken with your referees. If you are planning on needing them this year now is a good time to reconnect before the year starts to get away. just drop them a quick email to let them know your plans for 2019 and to remind them how they know you (some referees see a lot of trainee doctors so it can be hard to keep track).
3. Set Yourself A Plan
If you are planning on applying for a new job this year you probably know this already and know what you are aiming for. You will have some months before the interview arrives. Now is a great time to put a plan together.
Your plan should include at least the following:
Researching Your Next Position
Review the position descriptions from past years to see what the selection criteria are likely to be. Talk to current incumbents and supervisors. If it s a training position check out the College application requirements and try to talk to the Director of Training.
Preparing and Submitting Your Application
You should allow time to fill in the job application. Again you may be able to find information from past years that gives you a guide to how this will work. You will also need time to review your CV. More on this below.
Interview Practice
Interview practice is the most important part of your plan. You should allow plenty of time to prepare for the interview and practice potential questions.
4. Enrol In That Short Course
There are lots of short courses that can help you improve your application (for example advanced life support or trauma courses). Particularly for trainee roles. If you are already in training you might be considering an exam preparatory course. Getting leave approval for these courses may be difficult and sometimes the course numbers are limited.
Now’s the time to book that course and get your Manager’s approval to attend. Your Manager will love you for being proactive.
5. Prepare or Refresh Your CV
Any doctor job application CV should where possible be tailored to the post. This takes time (although sadly in many cases not long to be reviewed). You may never have had to put together this document before so this will likely increase the time required further.
It also can be confusing what the difference between a CV and a Resume. Even though employers ask for a CV they really mean something closer to a resume.
Getting a BPT position can be highly competitive. Especially in some of the premier programs.
Here’s a collection of the basic physician training interview questions we have gathered to help you in your endeavours.
Basic Physician Training Interview Questions
Basic Physician Trainee (BPT) Interview Questions
Clinical Scenario Questions
A 70-year-old patient presents to a rural Emergency Department with acute chest pain. Past medical history includes a renal transplant and type 2 diabetes mellitus. On assessment, BP is 70/40 mmHg and the patient is diaphoretic.
Outline your assessment and management approach.
ECG shows narrow complex sinus tachycardia – what do you do now?
A 92-year-old patient is brought to the Emergency Department from a nursing home with a GCS of 9.
How would you go about gathering the history?
A woman who has been feeling unwell for several weeks to months presents with a creatinine of 600 µmol/L.
What is your approach?
What are the indications for dialysis?
A patient presents with heart failure and anuria.
How would you assess and manage this situation?
An 87-year-old man with vascular dementia presents with a diabetic foot ulcer and fever. His wife, who is frail, feels unable to care for him at home. The patient expresses concerns about their relationship and the suggestion of nursing home placement.
How would you assess and manage this complex social situation?
A patient with poorly controlled diabetes presents with a foot ulcer under the great toe.
Outline your approach to assessment and management.
A 62-year-old patient with metastatic colorectal cancer presents with new onset shortness of breath.
What are your differential diagnoses and how would you manage the patient?
A 62-year-old patient with metastatic prostate cancer presents with lumbar back pain, constipation, abdominal pain, and confusion.
What are your differentials and how would you manage this patient?
A woman with metastatic breast cancer presents with haematemesis, hypotension, and tachycardia.
How would you assess and manage her?
She arrests before the consultant is called – what do you do now?
A 60-year-old renal patient on the ward is reviewed during a clinical review call for reduced urine output. They are hypotensive, hyperkalaemic, clinically dry, with a high anion gap acidosis on ABG, and report chest tightness. No ACD in place and not previously on dialysis.
Describe your approach.
ICU is called – what would you say to them?
Family arrives – what do you say?
How would you discuss an advanced care directive?
A stroke patient is reviewed on the neurology ward. He has deteriorated over the admission and now has new fevers and is unresponsive to voice. No ACD is in place.
How would you proceed with management?
You are called to a postoperative patient who has collapsed. You are the most senior doctor on-site.
What is your management and differential diagnosis?
Ethical and Professionalism Scenarios
You are a first-term BPT. You find your supervisor difficult to approach, often unavailable during usual hours, and making decisions you don’t always agree with.
How would you manage this situation professionally?
You are a registrar on the haematology team caring for a patient who is not of English-speaking background with end-stage myeloma and severe back pain. The family refuses opioid analgesia, fearing it will hasten death.
How would you manage this ethically and clinically?
You’ve diagnosed a patient with terminal pancreatic cancer. A family member, concerned about cultural expectations, requests that the diagnosis not be disclosed to the patient.
How would you handle this situation, balancing ethical and cultural considerations?
You’ve noticed that a fellow BPT is frequently late, appears withdrawn, and their clinical performance seems to be affected.
How would you approach this situation while ensuring appropriate support and patient safety?
You notice a colleague is overworked and stressed in a busy rural hospital.
What steps would you take?
Your consultant is being harsh to your intern, who is very upset.
How would you address this situation?
Neurology-Focused Questions
A patient with motor neurone disease presents to ED in respiratory failure.
How would you approach this situation?
A patient with myasthenia gravis reports a sensation of something stuck in their throat.
What is your differential? Do they require admission?
Some people say neurology is too hard.
What would you say to convince them otherwise?
Tell us about a development in neurology that interests you.
Why do you want to pursue a career in neurology?
Personal and Reflective Questions
Tell us about a mistake you made in your career and what you learned from it.
Tell us about a difficult time in your life and how you managed it.
Tell us something non-medical about yourself.
What would you be if you weren’t a doctor?
How do you manage stress?
How do you relax?
Tell us about a time you experienced conflict in the workplace and how you resolved it.
What qualities do you possess that make you a good leader?
What skills or qualities do you possess that make you a good physician?
Training and Systems Questions
What is a physician? What does it mean to be a physician? What are the qualities of a good BPT?
What do you understand the role of a BPT to be?
What do you know about the RACP PREP program?
What are the roles and responsibilities of a BPT?
Why do you want to do BPT at [Hospital]?
Why have you chosen to do BPT in the [Network]?
What do you have to offer to our BPT program?
Where do you see yourself in five years?
Which medical professional you’ve worked with do you admire most, and why?
As part of the BPT program at [Hospital/Network], you are required to complete at least three months in a rural location.
Are you willing to go? Why or why not?
What would you change about the healthcare system?
What are the pros and cons of AI for Phyiscians?
How can the healthcare system become more sustainable?
What do you understand by the term Clinical Governance?
Need Help in Answering These Questions?
Join over 700 satisfied students on our comprehensive interview skills course
In 2015 the Review of Medical Intern Training Report, which was commissioned by the Australian Health Ministers’ Advisory Council had the following to say about the current state of medical internship in Australia.
[Internship in Australia] “should have entry requirements that reflect agreed and defined expectations of work-readiness that [medical] graduates must meet before commencing [their internship]”…
Final Report Independent Review of Medical Intern Training Tweet
…“there is scope to better facilitate the transition from university to practice by ensuring graduates are more consistently work-ready.”
Final Report Independent Review of Medical Intern Training Tweet
All well and good.
But what is exactly meant by work readiness?
Medical Education is unfortunately burdened oftentimes with a definitional problem. By which I mean if we have not established our terms and the majority are in agreement we have hobbled our chances of implementing an evidence-based approach from the get-go. Or as Dr Jason Frank puts it:
“Despite recent proposals to enhance the evidence base of medical education in general, progress is suboptimal. Without a common language in the medical education enterprise, educators and policy-makers are hampered in their attempts to pursue quality, ensure outcomes, evaluate policies, and further innovation” Toward a definition of competency-based education in medicine: a systematic review of published definitions.
Jason R. Frank, Rani Mungroo, Yasmine Ahmad, Mimi Wang, Stefanie De Rossi &Tanya Horsley Pages 631-637 | Published online: 27 Jul 2010 https://doi.org/10.3109/0142159X.2010.500898
So what is the definition of work readiness for interns (medical graduates)? Well, it turns out that there is none. Or at least not in the 1500 medical articles that I searched through to find one. Even the more researched and similar concept of preparedness seems to lack a framework or definition according to Monrouxe et al (2017) .
No wonder then that various stakeholders might have differing opinions on what constitutes a work ready graduate. From the graduate themselves who, if we translate the research in preparedness, we might expect around 2 to 3 out of ten to feel non-work ready. To the supervisors and directors of training who might in turn worry about whether 1 or 2 out of a hundred might have some deficits in work readiness. To the employer who sees the extreme cases of non-work readiness and is then at risk of attributional bias in suggesting that there is a more global problem. To the regularity authorities who see even fewer cases.
But we are of course talking binary concepts above. We are suggesting that a medical graduate is either work ready or not. Of course this is unlikely to be the case. From the research in nursing of Walker building on the work of Caballero we are told that
Work readiness is the degree to which graduates possess the characteristics and attributes that prepare them for success in the workplace…the consensus is that it is multifactorial [with the following dimensions identified] work competence… social intelligence… organisational acumen… personal work characteristics
In my own institution we are currently facing a challenge in endeavouring to implement a new medical degree with a stronger emphasis on a work ready graduate (in the absence of a definition of what one is). We know from talking to our current final year students and well as from external groups such as the Australian Medical Council that we could be doing better to prepare our students for the transition to internship.
But with an already crowded curriculum and teaching program delivered across a footprint the size of England with variable quality and reliability of technology what is the solution?
Well it turned out our medical students were keen to engage themselves in the problem and it also turned out that many of the intern and resident doctors working in our region were keen to pass on their knowledge and wisdom in a near to peer fashion. This resonated with the students. They wanted some practical advice for preparing for internship.
But how to connect the two? We had pockets were various face to face “Intern 101” programs were occurring amongst students and graduates but access was not consistent and as mentioned getting everyone together (even using University video technology) was not easy.
The solution was a personalised approach. Most medical students and graduate doctors use facebook as a form for connecting and sharing of ideas. Facebook is one of many applications that helps people establish personalised learning environments (PLEs). PLEs are now old concepts in education land but are still reasonably foreign in medical education. Milligan defines PLEs as thus
Systems that help learners take control of and manage their own learning. PLEs support learners to: set their own learning goals (possibly with the support of teachers) manage their learning, both content and process communicate with others in the process of learning
Most of what has been written about PLESs is in relation to digital technology and in particular dynamic web applications, other wise known as Web 2.0. PLEs are in fact a learning concept or approach and they don’t necessarily require digital technologies to exist. But there is no doubt that recent changes in the internet such as search and social networks has greatly expanded the ability of learners to engage in personalised learning (even if they are unaware that this is what they are in fact doing).
What We Did
We used a closed group on facebook to invite all current final year medical students as well as intern and resident teachers. We fielded suggested topics from both students and teachers. Once a month an hour long webinar occurred during the evening using Zoom webinar and Facebook Livestream to the group. Students could attend and ask questions in real time as well as share their own resources with others. If students did not wish to attend live or were unable to they could watch the webinar later and ask questions at this point. If students preferred not to use facebook we posted the webinars to the student group on their University Learning Management System as well.
By making the sessions relevant to the student we were able to have strong participation in the group and the webinars (98% of the cohort joined and some of the videos were seen by 85% plus of the group). The interns and residents were more available during the evening and were able to bring their own approach (i.e. some used PCs, some used tablets, some used power points, some had physical resources to display). Students and teachers connected independently of the university videoconferencing infrastructure and the system “just worked” like all systems should.
Even two years ago we could not have done this in such a fashion as whilst the technology existed the integration of a closed facebook group with livestream did not.
What Are the Implications for Faculty?
Harden and Lilley have suggested 8 Roles for the modern the Medical Teacher:
Scholar and Teacher
Professional
Manager and Leader
Assessor and Diagnostician
Curriculum Developer and Planner
Role Model as Teacher and Practitioner
Information Provider and Coach
Facilitator and Mentor
That’s a long list. But a couple of things I don’t see on this list are “Curator” and “Marketer”. Let me explain further. If we are to accept that learning in medical education is to progress down a path where the learner is more in control and has more options about what they learn, then being fixed in one’s personal teaching delivery is likely to lead to stagnation. In recent days if a new teacher was asked to take on a particular lecture topic they would often ask the old teacher for their slides. Nowadays you can hop on to YouTube and quickly realise that for most topics someone has already covered it usually in a better and more entertaining way. For example, Osmosis has over 800 explainer videos on a range of common medical school topics with over 800,000 subscribers!
Find Your Niche
This is not to say that there is not a role for new content. The trick will be for us as Medical Educators to avoid producing content that has already been well covered. To collect for our students (curate) content to make their task in finding useful resources easier. To create useful new content in our niche and to ensure that our students are aware of our efforts (marketing).
In my own personal example. I have noticed that doctors are poorly prepared for career transitions, for example putting together resumes and preparing for job interviews. Its an area I have knowledge about and interest in. So I have started a “niche” YouTube channel called Career Doctor with the Value Proposition of helping other doctors to manage their own medical careers.
Many of my most succesful videos to date have been what’s called “How To” videos. For example the How to Make a Stand Out Medical CV (Resume) video as of publishing this article has 1.1k views in less than 12 months.
I’ve been careful to ensure that my efforts to provide free teaching resources are not wasted by adopting best YouTube practices (good titles, good thumbnails, tagging etc..) as well as promoting broadly on social media, using email marketing and of course setting up this particular website as a presence on the web to blog about these efforts.
Interestingly along the way I have found that some learners quite quickly adopt the ideas that I suggest in my videos, whereas others contact me after with questions as if they have not really watched the videos. In many ways this is an example of the “curse of the expert”. Putting in too much content or learning based on your own knowledge of the subject.
In other cases its possibly an example that some learners want to learn independently (learn from you), others want some form of coaching or interaction (learn with you) and finally some just want you to solve the problem for them (get it done by you).
This post was originally written as a flipped resources session for a teaching session I took with some Psychiatry Trainees.
The aim of this post and the teaching session is to touch on some practical issues in relation to becoming a better medical educator.
Presentations
There are many more bad presentations than good
Giving a presentation is a core skill for most doctors. It is something you are often requested to do, whether this be for some medical students, a Grand Rounds or a scientific meeting.
It is often said that there is a real “art” to giving a good presentation. But I’d like to call BS on that and suggest to you that actually its a science and we know a lot about what makes an effective presentation and most of the time we largely choose to ignore this.
Some resources you might find helpful include this wonderful TEDx Talk by David J Phillips on “How to Avoid Death By Powerpoint”. For me watching this video about 4 years ago was a game changer. It made a massive difference to my slide presentations, partly by paradoxically lengthening the number of slides (whilst reducingthe overall content). Before watching this video I had converted from powerpoint over to Prezi. But it turns out I was trying to solve the wrong problem. I thought that powerpoint made bad presentations. Actually its people that use powerpoint to make bad presentations. And to a lesser extent the default settings of powerpoint are also to blame.
Death by PowerPoint David JP Phillips
Another great resource just released by Queensland Medical Educator Kate Jurd is this eLearning Resource.
If I was to give my 4 top tips for more effective presentations they would be this:
Think firstly whether the presentation you are going to deliver will be enhanced by slides or whether it may be better (and more novel for the audience) if you don’t use slides. There are several other options, including just an oral presentation. I often find that if I have a good case prepared and perhaps a white board for demonstration purposes I can provide a more interactive and passionate and lively session.
If you must use slides try not make your last slide “Any Questions”. This just creates doubt and ruins any impact you have just made. Leave the audience with the key point and a Call To Action.
There are many great places to find creative commons licensed images to enhance a presentation. Pixabay is my general go to.
There are 4 principles that form a good starting basis to an effective teaching or learning session which I always give to new medical educators. They are FAIR and are from Ronald Harden. You can source them from the following text (available in many medical libraries and from me if you ever work as an Education Registrar or the like with me).
Feedback is fundamental as it can help to correct problems for learners, clarify learning goals and reinforce good performance (motivate learning). More on this later.
ActiveLearning has been shown to accelerate learning. By actively involving the learner in the process. By getting them doing things (rather than listening or observing) more cognitive processes are engaged. There are many options for “activating learners”. Here are a few ideas:
Find out what the learner already knows about the topic
Give the learner a problem to solve related to their new knowledge
Give the learner a test
Get the learner to carry out a procedure
Ask the learner to reflect on their learning
Ask the learner to share their knowledge with other students
Individualisation
Where possible make sure that the learning your are involved with is attached to a clearly accessible and understandable syllabus. A syllabus is a document that communicates course information and defines learning expectations. Done well it can translate the curriculum into something actually understandable by students (as well as most teachers!). And usually includes a list of resources for the students to use to help them in their learning
Provide a range of different resources in different modalities to assist learners. I often try to provide a mix of book recommendations along with blog posts and link to videos and where possible also examples of any assessments (if the course includes an assessment).
Provide opportunities for the learner to come back and repeat the learning exercise.
Relevance is particularly important in view of the ever-expanding mass of medical knowledge. There is a temptation for everyone to view their own component of Medicine as vital for everyone else to know about. Some strategies that clinical educators may want to apply to ensure that their teaching is relevant, include:
Asking the Learner. Medical Students and Trainee Doctors will be aware of the next gaps in their knowledge and have a reasonable view on what they are attempting to learn or master. Bear in mind that the learners view of what is important may not be the total picture and may often reflect what the learner perceives as the next steps in learning (see Zone of Proximal Development below) as well as what they think will be on the test.
Obtain Feedback from the Learner. Find out from the learner if what you are teaching and in the way you are teaching is helpful.
Find out what the learner needs to know. It is not uncommon to be confronted by a situation where there are learners who would like some impromptu teaching. In such circumstances, with no clear understanding of the curriculum, we tend to either ask the students or use our best judgement. This may lead to teaching and learning which is perhaps useful but not what the learner “needs” to know. If you regularly teach medical students or trainee doctors make enquiries about their curriculum, syllabus or learning outcomes. When you get your hand on a document like this find some things in it that you feel comfortable or passionate in teaching.
Feedback
Lets look at feedback in a bit more depth. Feedback is a core skill for anyone working in mental health. We use it constantly with our patients but its also an important skill for working with colleagues.
There are many models and approaches to feedback. There are none that really stand out in terms of being better than others. What is more important is how quickly or immediately you provide feedback. The closer to the activity the better as the student or learner will be able to better relate your feedback. As well as being specific. Although specific does not necessarily mean detailed. Sometimes you observe more than one thing that you would like to give feedback. Its often best to decide on the key piece of feedback. Be specific about that and leave the rest for another time. This helps to avoid “cognitive overload”. More about this below.
If you are starting out its probably a good idea to find a model that makes sense to you and use it. But bear in mind the need to be flexible in your approach.
To quote Michael a good summary of the research on feedback is:
(1) feedback is important, and (2) the quality of feedback varies widely.
Michael Gisondi
Psychological Safety
One important principle of feedback is Psychological Safety. It is a term that you may hear a lot if you are ever involved in Simulation Training. Psychological safety is a shared belief amongst members of a team that the team is safe for interpersonal risk-taking. It can be defined as “being able to show and employ one’s self without fear of negative consequences of self-image, status or career”. In psychologically safe teams, team members feel accepted and respected. It is also the most studied enabling condition in group dynamics and team learning research.
If you are wanting to establish a psychologically safe space with a new learner (someone you are not familiar with). Be aware that it takes time to do so. A good rule of thumb is you need to ask a novice learner 3 times if there is something they wish to learn or are worried about before they will take you seriously. So persist.
“I believe that trainees are intelligent, capable, care about doing their best and want to improve.”
Center for Medical Simulation, Harvard
Practice Your Feedback
Review some of the vignettes from the Teaching to Teach Series below and think about the process of feedback in each vignette.
First, think about the learner and what sort of feedback you would like to give them.
Then think about the teacher in the situation. How would you appraise their feedback skills? What feedback would you give them about their feedback?
The Intern – 3 Part Video Series
Teaching Medical Students
Learning Theory
In order to be a better clinical educator its worth knowing a little bit about educational theory. If you have read this post all the way through then you have already learnt some theory in relation to feedback, as well as Cognitive Load and Action Learning.
A great source to get started with Learning Theory is the ICE (International Clinical Educators) Net Blog which is supported by the Royal College of Physicians and Surgeons of Canada.
In this post you will learn that knowledge is constructed (often socially) rather than transferred and learning involves a process of building new knowledge on top of existing knowledge. So new learning is influenced by past learning experiences. Authenticity and emotion can be useful tools to improve learning and retention of knowledge. Along with regular challenges (assessments) to ensure embedding of knowledge.
You will also read in this post that contrary to popular belief matching your teaching approach to learning styles is definitely not practical and probably not based in sound evidence. And also that Adult Learning Theory is probably not a great theory.
The ICENet also did a series of 9 posts looking at other relevant Learning Theories which are worth making your way through:
Interviewing for a job as a doctor can be stressful, especially when its been a while since you may have had some practice.
A way that some doctors choose to improve their interview skills is to work with a coach. During interview coaching, a doctor meets with a professional coach to learn strategies for being more relaxed about the interview process and of course to perform better.
Should you work with an interview coach? And if so, how can you find a doctor interview coach in Sydney?
Why Interview Coaching?
The most obvious reason is that interview coaching can help increase your chances of getting a job. There are a number of ways this can occur.
Coaching can help you overcome any nerves or anxiety you have about the process. Coaching gives you a chance to experience answering many different interview questions. Coaches provide you with feedback to help improve your responses during interviews.The more you practice with a coach, the more confident you will become. By engaging with a coach you are also ensuring that you commit to your own practice regimen, which is important for a good performance.
Some reasons you may want to consider engaging a doctor interview coach in Sydney
It’s been awhile. If it’s been a few years since the last time you interviewed for a doctor job or if your last interview was fairly simple and you anticipate this one will not be the same, then a coach can help you rehearse and regain your interview confidence.
You get nervous before interviews. A little bit of anxiety is good going into an interview. But too much anxiety can affect performance. Practicing with a coach can help you feel more comfortable, relaxed and prepared.
You get interviews, but not offers. Often its difficult to get honest feedback from medical interviews. A coach may be able to help work out what is going wrong for you.
You are not sure about something on your CV. Maybe you have had to have a break in work. Or your last job didn’t go so well. Are you perhaps switching specialties. A coach can help you with how to tell the right story in relation to these sorts of issues.
Its your dream job and you want to land it. A coach can help with feeling confident in these situations.
On the other hand, if you’re a confident interviewer and have always tended to perform well during interviews, then a coach may not be necessary.
Types of Interview Coaching
There are many types of interview coaching. Some coaches meet with you in person, and others speak with you online or on the phone.In general interview coaches work on something called “performance coaching”. Think of it like a sports coach working with an elite athlete. A key element is practice with feedback. The more practice and the more immediate the feedback the better.
If you meet the coach in person or online, they can also help you develop effective visual communication. The coach can work with you on facial and body expressions that convey trust and show active listening.
Coaches may also help you with other elements of the interview, including how to ask the right questions of the employer, how to research the job and the panel and even some advice on how to
How to Find a Doctor Interview Coach in Sydney
There are lots of coaches available to choose from in a capital city like Sydney. Career coaches often offer interview coaching. Some things you should consider in a coach are the following:
What is their training and experience in interview coaching?
What sort of knowledge and experience do they have with the actual interview process. Medical interviews can be fairly unique, particularly in terms of the types of questions asked and what panels may be looking for. So someone who has actual doctor interview panel experience is ideal.
Do they provide face to face coaching or on the phone or online. Face to face may seem best initially. But consider that you may need to travel to see the coach and often during normal work hours. Phone coaching and online coaching may be more convenient and cut down on travel.
What feedback is provided after each session. Phone and online coaches can often give you a recording of the session for you to review.
What is the price of the coaching.
If you cannot afford a coach, there are some opportunities for less expensive or even free coaching. Your Director of Training may be skilled in interview coaching or may be able to recommend another Consultant in your hospital who is.
Coaching
For Job Applications || For Interview Practice || For General Needs
Excelling At Doctor Job Interview Questions And Answers
Recently I hosted a free Live Webinar on YouTube about the interview process. We had over 40 trainee doctors to help everyone get better prepared for their upcoming job interviews and how to answer doctor interview questions.
You can watch the full video above. But just in case you are looking for some specific guidance I have taken the time to timestamp it as well so you can find the information that you want more quickly. The timestamps are provided here on this post as well.
Also, another hack for speed watching YouTube videos on PC is that you can turn the settings to watch the video at up to 2x speed.
Introduction & Webinar Outline
Logistics
In this section we cover a little bit about dress code, finding out about the interview style and panel, getting your documents together and working out how to get to the interview. The key emphasis should be to deal with these practical matters as quickly and soon as possible so you can focus in on your interview.
Multiple Mini Interviews
An emerging trend in doctor interviews is that of multiple mini interviews. We cover what these are and how they may differ slightly from the traditional one panel interview and therefore what sort of doctor interview questions you should practice.
Review Your CV & Don’t Forget to Smile
Its always a good idea to review your CV prior to your doctor interview. Similarly practicing your smile can make the doctor interview question and answer process a more relaxed one for you and the panel and help to give a positive vibe.
Interview Frameworks for Doctor Interview Questions
There are two Frameworks I recommend you learn which will help you with 99% of the questions
Specific Doctor Interview Questions:
a. Tell Us About You?
b. Why You (for the Job)?
c. Strengths and Weaknesses
d. Work Conflict
e. Ethical Dilemma
f. The Do You Have Any Questions? Question
Discriminatory Questions
Some Final Thoughts on Practising Doctor Interview Questions
I hope that this video is helpful to you. Leave a like or comment on YouTube or below if it is. Think about subscribing if you want to enjoy more helpful content.
But what do you do if someone asks you discriminatory questions (in the middle of an interview for a medical job that you really want)?
Last year there was much discussion (and rightly so) about the topic of discriminatory selection practices and illegal interview questions that occur in medical training. We wanted to write a post to remind both panel members and candidates that there are certain questions that you should not ask in an interview.
But we also wanted to give some advice to candidates about what you should do if it happens. This is because sadly these sorts of scenarios remain common-place in our profession. Something we found out when we put out the call on social media for other doctors to share their experiences about discriminatory interview questions. We were inundated with responses. We have included a select number of deidentified quotes in this article to illustrate the point. It probably does not need to be pointed out but by far the majority of doctors we talked to who reported a problem with inappropriate or illegal interview questions were women. That being said, this can and sometimes does happen to anyone.
For a Basic Physician Training interview:
Interviewer: “What else have you done besides have a baby?”
(as well as whether I was planning on another one and informing me that no time off in BPT was allowed and I would have to start again).
The women on the panel looked appalled.
In the preapplication information night the audience were told “no breaks in basic physician training unless you get pregnant with twins or develop lymphoma!”
Yep I’ve been asked if I planned to have kids in an interview.
They tried to soften the blow by prefacing it with – I’m not allowed to ask this but…..
Things they are not allowed to ask you – what are the illegal interview questions?
Let’s just get this bit right out of the way first. There are a number of areas that according to Australian law are “out of bounds”. The basic principle is that questions should only be used to discriminate between applicants when they relate to the candidate’s actual ability to perform the job regardless of other personal circumstances. Asking other types of irrelevant questions at interview may disadvantage some people and could amount to discrimination.
Employers are required by law to ensure that discrimination does not occur when recruiting staff and this responsibility extends to ensuring that those involved in the selection process avoid asking discriminatory questions. In other words, employers are liable for the actions of the members of the selection panel. Discrimination is illegal unless it is relevant to a person’s ability to perform the inherent tasks of the role. Discrimination is specifically against the law in Australia if it is based on a person’s
age
disability
race, including colour, national or ethnic origin or immigrant status
sex, pregnancy, marital or relationship status, family responsibilities or breastfeeding
sexual orientation, gender identity or intersex status
So, questions like: “Do you plan to have children?” and “Do you really think you can complete training at your age?” are clearly not permitted and are illegal interview questions.
For a job as a GP registrar in a rural town:
Interviewer: “Are you single?”
(I was)
Interviewer: “Would you like a hand finding a nice local boy to settle down with?”
(I politely declined)
Other areas of possible discrimination
But it does not stop there, under the Australian Human Rights Commission Act, individuals can also lodge complaints with the Commission concerning discrimination in employment for a number of other reasons, including religion, political opinion, national extraction, nationality, social origin, medical record, trade union activity and even your criminal record.
While interviewing for entry onto the GP training program:
Interviewer: “What did you do with all your time on maternity leave?”
(I was proud of myself for completing the Diploma of Child Health during that period, so thats what I said)
Interviewer: “Yeah and what else?”
Interviewing for GP training. The Director of Training during a teleconference meeting, planning my training DOT: “Older trainees find it hard to settle down into training”
Grey Areas
A blatantly discriminatory question can and sadly still does happen. In some situations, it’s a case of the interviewer not knowing better. But some do know and have also “wised up” to this and invented new and clever ways of finding out information about your personal details.
The pre-interview small talk can be an area of danger. Some panels like to make candidates comfortable by kicking off with a bit of banter prior to the first actual question but this can often stray into the “tell us a bit about yourself?” question, which can then often lead into more personal topics such as “what does your partner do?” or of course a range of questions about children.
Interviewer: Where are you from?
Me: I grew up in Western Australia
Interviewer: No…what’s your background?
Me: My genetics? It’s a mess. Bit of everything but mainly a combination of communist and terrorist.
Interviewer: (Stern unimpressed frown)
Me: I guess I’m a world citizen with an Australian citizenship.
This was at an interview for O&G training an offer which I didn’t take up.
In the formal part of the interview, someone experienced will normally vet the set questions. But there are still certain questions that interviewers can use to “fish” for information or as a chance to ask a “follow-up” question of individual candidates.
Coping with the Stress of the Job?
One question we hate particularly, for a whole host of reasons is: “How will you cope with the stress of this position?”
First of all, we should all be working hard to make sure that we make the job experience in medicine more civilised, so we don’t have to ask a question about coping with stress. But more than that in most cases a “good response” to this question would include an outline of social supports and how one balances work with other responsibilities. Which very handily gives the person asking the question the opportunity to probe a bit deeper into each candidate’s personal circumstances.
What should honest panel members be doing to prevent discrimination and illegal interview questions?
The first piece of advice we would give is “know the law”. Know what is discriminatory and know what you should not be asking about and why? Most employers will offer training in recruitment and selection its wise to attend this as they will generally cover in depth equal employment opportunity.
The second piece of advice is to be aware that others on the panel may not be as well versed in “what’s ok to ask and what’s not ok”. Sadly, not everyone who sits on a panel has undertaken the correct training. Make sure you step in and guide another panel member if they are straying into inappropriate territory.
I’ve never been asked inappropriate questions but have had (on two separate occasions) older male interviewers say casually racist things (I’m Caucasian). Do they assume it’s ok to speak that way when there’s only white people in the room?
I was interviewed by a panel of 3 male GPs and as a closing question one asked if I was planning on having any more children, thankfully he was shut down by the other two before I had a chance to answer.
Panel members should step in to prevent illegal interview questions.
So many of the anecdotes we heard were about other panel members being uncomfortable but choosing not to step in. Candidates are looking to know if it is just an isolated “dickhead on the panel” problem. Or a more systemic cultural problem with the whole program. So what you do in this circumstance definitely does matter.
At my first Consultant interview one of the Consultants was a good female friend. She deliberately asked me about partners and pregnancy to see if it was challenged by the rest of the panel. Because this had happened to her at the same interview a few years prior and she had called them on it. I quoted all the reasons why it was none of the panel’s business and they all blustered an apology. We both had a good laugh about it afterwards as we celebrated with coffee. Didn’t happen to any of other female Consultants after that!
What should you do if confronted by an illegal interview question?
Of course, you can just tackle the question head-on and point out to the panel that it is inappropriate. You might also ask them which selection criteria it addresses (they probably will not be able to answer). But there may be a number of reasons why you don’t feel empowered to do this. From feeling disempowered. To not expecting the question. To really wanting the position and not wanting to put the panel offside by engaging in a conflict with a panel member.
A better strategy for many is to deflect the question by ignoring that part of the question which is discriminatory and focusing on the appropriate parts.
Deflecting the Question.
Sometimes this might require you to think a bit more about the rationale behind the interviewer’s question. For example, you might receive an initial question about the challenges of the position and your availability to work after hours shifts. A follow-up question might then centre around your childcare arrangements. This question may well stem from the interviewer’s concern for you and your family’s well-being OR it might just stem from a more self-centred concern about filling the roster.
Whilst a candidate can outline the panel their childcare arrangements in detail and go over the fact that they spend at least 2 hours a week coordinating diaries with their partner. The panel actually has no need for this information. Instead, you might respond by pointing out that in your last 3 appointments there were never any concerns about your ability to show up for work on time and participate in your share of the overtime roster. Thus, bringing the discussion back to job-related qualities.
Do you foresee any problems?
Another question that can commonly be used to discriminate against candidates is: “Do you foresee any problems in fulfilling the requirements of the position?” This question is obviously probing for a reason why a candidate might be at risk of not completing their contract. The two big reasons why this might be the case are health-related and pregnancy-related. Again. We have to stress that both health and pregnancy are personal matters. Ones which employers are not able to discriminate against employees. Moreover, employment law requires that employers make provision for employees requiring sick leave and maternity or paternity leave.
So you don’t actually have to tell them about any plans you have for children or any concerns that you might require sick leave as you will actually be able to take leave under your contract for these things. Instead, we suggest just answering this sort of question with a simple “No. I don’t foresee any issues with fulfilling the requirements of the position.”
The panel asked me the question of whether there was any reason that I was going to take time off the following year. I just told them right back that they couldn’t ask me that! They just all chuckled and said they just needed to organise the year.
What should you do afterwards?
Ok. You’ve managed to survive the interview. You are probably feeling either uncomfortable, anxious or annoyed or a bit of all three. These feelings may also turn into feeling conflicted at some stage. Especially if you were pinning your hopes on the job you were applying for. At this stage it’s a good idea to talk to someone else, be it a friend, a family member, a mentor, a union official or a lawyer. Something you may have to decide is whether you now want the job if it is offered to you. Or to put it another way is the job really worth it?
What you have just encountered is a red flag. A sign that all may not be well with the culture of the team you are potentially about to join. This probably requires further research. Many candidates may already have some awareness of the culture of the program or department they are applying to join. They may have worked in the same location already. Others will probably need to ask around, particularly of other current trainees. One possible big indicator is whether other panel members interrupted or at least looked uncomfortable when the person who asked you an inappropriate question asked you that question.
Consider Lodging a Complaint.
As a medical trainee you can always complain about the situation. There are many avenues for doing this. Firstly, you may wish to contact the hospital directly to let them know what has happened or contact the hospital Human Resources Department. Secondly, you may wish to contact your union or the AMA or speak with a lawyer. Finally, you can contact the Australian Human Rights Commission. If you are offered the job and decided to turn it down. You might wish to indicate that the interview process was part of your reason for declining.
Thank You
We would like to thank the many doctors who responded to our request for stories on social media. We are sorry that we cannot print all of them.
I wasn’t asked this in the interview. But one of my referees was asked if it was true that I had a child
I had my 35 week pregnant tummy patted by the interviewer
Interviewer: ‘What do we have here?…How do you plan to feed the child?…Who is going to look after the child?’
I did not get any questions relating to my job
Anthony Llewellyn
FRANZCP, MHA, GAICD | Medical HR Expert and Coach. Anthony is an experienced health public sector executive, medical educationalist and coach. Anthony is an expert in Medical HR. He has reviewed numerous CVs, chaired and conducted over a thousand job interviews and provided advice to a number of employers and Colleges about selection processes. Anthony’s background: Consultant Psychiatrist and Medical Manager with 20 years’ experience as a medical practitioner in public health services in a range of roles. From 2012 to 2016, Anthony was the Medical Director of the Health Education & Training Institute (HETI), involved in overseeing a number of network training programs. He is also a Senior Lecturer at the University of Newcastle’s School of Medicine & Public Health, and Year 5 Psychiatry Coordinator. He is currently completing a PhD in Medical Education, exploring personal learning environments in the intern training space. Anthony recently delivered for the Royal Australasian College of Physicians a Best Practice Guide for Trainee Selection into Employment Roles Anthony was born on Mouheneenner land in Hobart (Tasmania) and pays respect to the traditional owners of lands he lives and works on, and elders past and present. His most important role in life is proud father of two boys.
Amandeep Hansra
Digital Health Leader | Evermed Consulting Dr Amandeep Hansra is a locally trained specialist General Practitioner who has worked both nationally and overseas and continues to work in clinical medicine at a General Practice in Bondi, Sydney. She has a passion for startups and supporting women in Medicine and was awarded “Women Leading in Business Scholarship” for the Global Executive MBA at the University of Sydney.
Her past career has included both public, volunteer and private work, as well as in Aboriginal Health, Refugee Health, Occupational Medicine and Travel Medicine. She is a Fellow of the RACGP, an examiner for the College, holds a Master’s in Public Health and Tropical Medicine, the Australia Certificate in Civil Aviation Medicine, mentors junior doctors through the AMA and has completed the Company Directors Course through AICD.
Amandeep is a leader in digital health and telehealth sevices in Australia. Amandeep co-founded Evermed Consulting and provides consulting services to insurers, start ups, health service, investors and businesses. She was most recently the CEO & Medical Director of Telstra’s telemedicine business ReadyCare; a joint venture between Telstra and Medgate, Switzerland’s leading telemedicine provider. She also served as the Chief Medical Officer for Telstra Health and separately has assisted Medgate in setting up a telemedicine business in the Philippines where she remains the Chair of the Clinical Advisory Board.
The Implications for Medical CV design, structure and content
We recently hosted an evening webinar on the Medical CV. 70 trainee doctor registrant learnt how the selection panel reviews your Medical CV.
Trainees are often surprised when they find out how little time is spent looking at their Medical CV at each stage of the process (in some cases a few seconds to minutes). This is probably even more shocking when trainees often spend hours putting one together.
Generally speaking, there are 3 phases in which your Medical CV is considered post submission.
Stage 1 Initial Review of your Medical CV
This is often done by only one person (usually the Chair of the Panel). The process can literally be a few seconds per CV. The main purpose of this stage is determining who should be interviewed and who should not. This is sometimes referred to as shortlisting or culling. Your main aim at this point of the process is for your CV to provide all the essential information required to get into the interview pile. Standing out is only a secondary aim. So make sure you have reviewed the job description and put all the essential stuff that may be required, such as medical degree, registration status, years of experience, trainee status somewhere on the front page, preferably in either the header or the career goal section.
Stage 2 Pre Interview Review of Medical CV
This is when the other panel members have the opportunity to browse your CV prior to the interview day. Some will do this in more depth than others. It’s your first chance to stand out. So again a good career goal statement and a well laid out CV is essential at this point. Because they are just browsing again the front page should include all the main things you want them to know about you, as they are only likely to glance at the rest at best.
Stage 3 The Interview
Your CV (and application) will probably be sitting amidst a pile of others in the interview room so that panel members can refer to it. So why not refer to it yourself in your interview responses. This reminds the panel that its there and contains further information about you to support your candidacy.
For much more about how the panel reviews your Medical CV and the implications for structure, content and design see our video below, where we also talk about whether you need to do a cover letter or not.
We recently recorded a “how to put together a medical trainee CV video” (Resume).
There’s tremendous interest in the topic of how to put together a medical trainee CV. Medical students are also interested in the topic. For many, it may be the very first time you have have to assemble a CV or resume.
That’s why we put the call out via email and our facebook community group (lots of good stuff in there to help you with your medical career in there by the way) for folks interested in a webinar on key points for putting together a good medical trainee CV that will satisfy the needs of employers.
So a few Mondays ago, we held a Webinar of around 40 trainees and medical students to discuss some of the key aspects of putting together your CV.
So here it is:
How to Put Together a Medical Trainee CV video
This is a long video but we encourage you to watch it through entirely. By the way On Youtube, you can adjust the speed settings to listen a bit quicker if that works for you.
A bit of a summary of what was covered in this post (all the headings here link to sections of the video if you want to fast forward):
Search for more than a couple of minutes on the internet for information about CVs and you will find someone who tells you that the average first pass review for a CV is 6 seconds. I suspect many of these folks don’t even know where that reference comes from. Well, here it is. The study was an eye-tracking study and whilst its got its criticism and there’s a bit of a lack of detail. The study certainly meets face validity when you talk to people who are experienced with reviewing hundreds of CVs. When you are reviewing applications as part of an annual medical recruitment process its not unusual to receive hundreds of CVs. If you dig a bit further into the article, however, there’s another interesting finding.
If you were looking for an additional reason why you should not include a photo the study provides you one. I generally advise against photos on CVs for the following reasons. 1. Medical job applications tend to be conservative affairs. 2. It can come across as a bit narcissistic. 3. It also removes a key opportunity to make a first impression. If someone can see a picture of you, then they are already forming all sorts of biased opinions about you based on this photo.
But the Ladders study adds another reason not to do it. It distracts the attention of the reviewer from other more important information.
Personal Details (include a brief qualification summary)
Career Goal Statement
Work Achievements
Education Achievement
The Rest (in whatever order represents you best)
Referees
Why not Education before Work? Because this is an employer interview and that’s what is of most interest.
There are some circumstances where Education could or should come before Work. This is generally when you have been educating more recently than working, for example still in Medical School or an International Medical Graduate.
If you look at these templates they are not overly attractive. Filling one in will mean that yours looks like everyone else’s’. So its hard to put together a medical trainee CV that stands out in those circumstances. All these templates are really trying to achieve is that you provide the reviewer with a minimum amount of information. So you can refer to them and still adopt your own style. So far, everyone I have reviewed in Australia and New Zealand is published as a guide (meaning you don’t have to use it). Feel free to send me one that is not but so far I have looked at:
In general, its good to talk about any substantive work you have done in a previous life outside of Medicine. Where you list this will depend on other work history and education and how much of a strength you feel this is. You can also cross-reference some things in other headings like Skills or even the career goal statement. For example, if you were previously an Executive Assistant then you have definitely done a job in the past that required high level organisational, time management, stakeholder management and communication skills.
Try to give some evidence for what you have achieved in your past roles. Avoid listing common job responsibilities this will bore a CV reviewer. They already know what OR at least think they know what an Intern does on a day to day basis.
3 is good. But remember they will be contacted in the order you put them. And the 3rd is only normally contacted as a back-up if one of the other two goes missing.
You can have more. But probably more than 5 or 6 is starting to look excessive.
The biggest take-home message here is. GET SOMEONE ELSE TO REVIEW YOUR CV FOR YOU. Attention to detail in CVs is important. You have probably spent a few hours putting it together and revising it. You will probably now be overlooking a typo or formatting error.
The Audience Q&A included a discussion about Cover Letters and Personal Statements. For Personal Statements, I generally recommend a Career Goal Statement instead. I will at some point try to write a post or do a video on Cover Letters.
A Quick Reminder about the YouTube Channel
I’ve decided to start a Youtube Channel. I really would like to share with a wider audience some of the knowledge that I have gained over several years doing jobs in Medicine that I really love. But let’s face it most other doctors really hate. I’m talking about things like medical manager roles, executive leadership roles, recruitment roles, coaching roles, committee roles and clinician engagement roles. So some of the stuff I know is fairly unique. I also have a network of peers that could contribute useful information in the broad are of doctors careers.
So I’ve started out vlogging on a couple of topics.
One is about the idea that if senior doctors could become better bosses (people managers). And if trainees could understand that being a boss is quite difficult at times. Then we might have a positive impact on the culture of medicine.
The other topic. Quite relevant at this point in time. Is the one we have been talking about. The job application and interview preparation process.
My current goal is 100 subscribers by the end of July. As of the time of writing this post I was sitting at 40. Why 100? Well, that’s the magic number at which point Youtube lets you have your own custom channel name.
So if you feel inclined you could really help me out by doing any or all of the following (none of which will take up more than a small amount of your time):
Those who know me know that I am a big fan of Robert Sutton‘s classic book on Workplace Civility (The No Asshole Rule). In this book Sutton demonstrates how one bad egg can have such a devastating effect on workplace culture and harmony. Including, yes you guessed it! Hospitals, where the difficult boss in medicine can and does exist.
That book dealt mainly with how organizations can detect if they have an asshole problem and how to deal with it if they found one. On its tenth anniversary, Sutton has published a follow (The Asshole Survival Guide) which is more of a personal help aid if you encounter a jerk in your workplace.
The main purpose of this post is not, however, about Assholes in Medicine. Its about that Difficult Boss in Medicine. The Consultant or Trainee who sometimes might be temporarily labelled an asshole (sometimes even fairly) for some of the things they do or don’t do. The folks who are not deliberately trying to up set others and who are generally well-meaning. These types of Bosses are much more common than the true workplace asshole but can still create grief and concern for those who work with them.
Bosses shape how people spend their days and whether they experience joy or despair, perform well or badly, or are healthy or sick. Unfortunately, there are hoards of mediocre and downright rotten bosses out there, and big gaps between the best and the worst.
Robert Sutton – Good Boss, Bad Boss: How to be the Best…and Learn from the Worst.
Is the Difficult Boss in Medicine a real problem?
I think the majority of medical trainees would answer yes to this question. In my own research 17-20% of medical trainees reported bullying and sexual harassment in the last year, with 60% of this coming from senior medical staff[1]. And of course bullying and sexual harassment is at the extreme end of difficult or bad bossness!
Perhaps part of the problem is who is a boss in Medicine? Registrars or Trainee tend to refer to their Consultant as “their boss”. Interns and Residents do as well, but then report on a daily matter to their Registrar. Very few of these Consultants or Registrars however have the title Manager or Director or something equivalent. So we have lots of bosses but most of them are not formal bosses. And many Consultants also speak openly about not wanting to be a boss.
I think that’s a real problem. CanMEDS has recognized that at the core of every good medical practitioner is the need to develop a level of Leadership and Management capability, along with other useful “boss skills” such as Professionalism and Communication. Colleges have started to pick up on this in training but sadly a focus n Leadership and Management skills still tends to come late in the curriculum.
When I talk to Advanced Trainees about their worries about transitioning to the Consultant level they tell me that they are not concerned about how to handle clinical problems as a boss, they are concerned about how to handle management problems (mostly people management).
So if we are not adequately preparing doctors for becoming a boss and have systems where nearly everyone becomes a boss at some point is it such a surprise that many are on what Sutton call the “mediocre to rotten” end of the spectrum?
So how many Types of Difficult Bosses in Medicine are out there?
The short answer is too many to describe in a blog post.
The longer answer is that not all Bosses are the same to all medical trainees.
An example of this is what I call the “Micromanager Boss“.
The Micromanager is concerned about avoiding risks and problems with their patients. They tend to have problems trusting others to ensure that what needs to be done is done (problems with delegating). They can be a great source of frustration for an experienced trainee as, despite your best effort, the Micromanager always seems to be wanting you to check or confirm something.
For an experienced trainee a Micromanager becomes a headache and you may start to resent their presence as an annoyance on the Ward. But consider this. What if you are an Intern who hasn’t reached that level of feeling experienced enough to know what to do? All of a sudden the Micromanage Boss becomes the Caring and Nurturing Boss. The Boss who goes the extra mile to make sure you have covered all the things that need to be done for the patient.
First seek understanding.
The point here is that in order to understand the Difficult Boss Problem you both need to understand yourself and your needs as a trainee. Try to understand the perspective of the Boss at question. If possible own your Difficult Boss in Medicine problem.
In our example above it may very well be that our boss has had some very bad outcomes in past. This may have been through a failure to check certain things with patients. OR perhaps under pressure from their own bosses to ensure that some things are done in a certain way?
So one strategy for overcoming your difficulties with your boss might be to seek further information about the source of the insecurities. Perhaps you can engage with them directly. Perhaps a previous trainee or one of the experienced nursing staff can shed some insight. If you can learn about what makes your Boss anxious you can take steps to reduce this. For example, by presenting them with a personal report each day showing how you have checked all these important things. Show them you have their back!
A couple of other examples of Difficult Bosses in Medicine, including possible reasons and how to own the problem:
The not so helpful boss.
Presentation:
This is the Boss that believes in old school teaching, likes to put you on the spot in the middle of the Ward round and quiz you on the 31 causes of hypertension.
Possible Reason:
This Boss may be very keen to teach and believe what they are doing is helpful. They may never have been taken aside and told that their teaching approach is no longer considered the best.
How to own it:
May be a difficult one to tackle front on. But perhaps if you are more observing this Boss interrogating another colleague you may feel able to take them aside for a private conversation. Otherwise, it might be useful to share with your Boss what you are currently studying and suggest that they could help you to focus on learning this (rather than anything that just happens to come up on the Ward Round).
The too nice boss.
Presentation:
This is the Boss who says yes to anything anyone, staff and patients because they seemingly “don’t want to upset anyone”. They leave you frustrated because a lot of those “yesses” mean you have to do extra things. Like an extra day on take, reorganizing a theatre list, or negotiating with a frustrated secretary about cramming extra time into an outpatient clinic.
Possible Reason:
Your Boss may be very new to the role and unsure of themselves. They may be wary of establishing credibility with their peers before saying no to things.
How to own it:
Such a Boss may be very receptive to a friendly empathic conversation about feeling new and unsure. Make it clear that you are happy to support more firm decisions when they are needed. But also make clear what you need to get your job done and what you may need from a boss. If possible see if there is another person around who can help with these but make sure that your Boss knows about this.
How to not become a Difficult Boss yourself.
Its never too late to avoid becoming known as one of those Difficult Bosses in Medicine. Of course you can learn the science and art of Management in Medicine by enrolling in a University Management training degrees. But there may be something a little shorter on offer at your local hospital. To be perfectly honest they are more likely to tackle the issues of how to be a good boss to your team members than any Masters degree course will.
Seek Feedback.
An even better start is to think about how well you are currently receiving feedback on your style as a leader and manager from those who report to you. Do you encourage feedback? Are you regularly receiving feedback? Is it the type of frank and fearless feedback that really opens your eyes to the need to change something you are doing?
We are generally very bad at evaluating our own performance. So its well worth considering formalizing feedback every few years by engaging in a 360 feedback process. Done well this process will normally give you one or two key areas for improvement as a people manager so you can avoid those below seeing you as “Difficult”.
Want to hear more about how to deal with a Difficult Boss in Medicine?
Llewellyn Anthony, Karageorge Aspasia, Nash Louise, Li Wenlong, Neuen Dennis (2018) Bullying and sexual harassment of junior doctors in New South Wales, Australia: rate and reporting outcomes. Australian Health Review, .https://doi.org/10.1071/AH17224