One of the most common requests I receive from International Medical Graduates (IMGs) on this blog or my YouTube channel is to explain the competent authority pathway process and/or answer who is eligible for the AHPRA competent authority pathway. There is a big reason for this. You see, the competent authority pathway is the most straightforward pathway for a doctor outside of Australia to gain work in Australia. Let me explain.
Competent Authority Pathway TL;DR
Any doctor who graduates from medical school in any of the four competent authority pathway countries and has completed the required one or two years of supervised experience is generally eligible to work as a doctor in Australia under a year of provisional registration. After which, if their performance is deemed suitable, they will be invited to apply for general registration. The four competent authority pathway countries are the United Kingdom, the United States, Republic of Ireland and Canada. The pathway is the best option for any trainee or prevocational trainee from these countries. IMG doctors from other countries can become eligible for the competent authority pathway by completing the USMLE, PLAB or LMCC process and obtaining the necessary experience. The PRES (Ireland) is not recognised by the Medical Board of Australia.
Doctors from the United Kingdom, Ireland, Canada and the United States have a strong track record of success in coming to Australia. These 4 countries comprise what is known as the competent authority pathway countries in Australia.
For example, for the years 2016 to 2021, 2077 UK Specialists were approved to work in Australia the next biggest group was specialists from India at 485.
And in the same time period many more UK, US, Irish and Canadian trainee doctors made the move to Australia during that time via what is called the competent authority pathway Australia.
So the prospects for working in Australia as a doctor from Ireland, the United States, the United Kingdom and Canada are excellent.
There is largely
New Zealand is not included in the list above as its medical schools are accredited by the same body as Australian medical schools – the Australian Medical Council. So doctors from New Zealand in Australia are generally treated identically (almost) as those from Australia. There is no need for a competent authority pathway New Zealand style, except for IMG doctors who qualify in New Zealand (see FAQs).
Historically UK medical qualifications have been recognized by the Australian Medical Council and the Medical Boards in Australia as being of high quality. The reason for this is quite simple. Australia inherited its medical training system from the United Kingdom, and to this day, both its undergraduate and postgraduate training systems remain pretty similar to those in the UK.
For this reason, again, Australia has recognized doctors from Ireland as having a higher quality. Because, once again, our training and regulatory systems are pretty similar.
The reasons why doctors from the United States and Canada are also recognised as being of higher quality are less clear. It is undoubtedly the case that these systems whilst somewhat different in their approaches to training are on par in terms of outcomes and the quality of health care in these countries.
An IMG doctor may, at this point, question why it is that these 4 countries are given priority status above other countries for the purpose of registering IMG doctors in Australia. This is, in my opinion a reasonable question. Unfortunately, there is no clear information about this on the Medical Board of Australia website. Nor does there appear to be a process for a new country to apply for competent authority status.
In any case, the main point of this post is to outline how an individual doctor can achieve eligibility and utilise this pathway.
Step 1 For Any UK Doctor Wanting to Work in Australia. Work Out Your Pathway.
The first step that any IMG doctor wishing to work in Australia needs to consider is which pathway they will be utilising. Often times you will be eligible for more than one pathway.
So, for example, a Specialist Anaesthetist, from the United States would in fact be eligible for all 4 pathways. Let me explain:
- They would be eligible to attempt the Standard Pathway (as this is open to all IMG doctors);
- They would be eligible to register via Competent Authority (as they achieved their medical degree in the United States and trained in the United States);
- They would be eligible for the Short Term Training in a Medical Specialty Pathway (as they are a qualified specialist); and finally
- They would be eligible for the Specialist Pathway (as they are a Specialist IMG), and this is, of course the pathway they would most likely be opting for.
As a side note, even if you are a Specialist from a Competent Authority Pathway country, you end up being registered via your Competent Authority status and are given provisional (as opposed to limited) registration as your first registration.
In summary, if you are a trainee doctor from any of the Competent Authority countries, you should choose the Competent Authority pathway. There are no advantages to the other 2 pathways.
And, if you are a Specialist IMG doctor from any of the Competent Authority countries, you should choose the Specialist pathway. Unless you are certain you only want to come to Australia to train for a limited period of time. In this case, choose the Competent Authority pathway as it will allow you to stay longer than the maximum period of 2 years under the Short Term Training pathway.

Competent Authority Pathway Course
A Free Course For Trainee Doctors
This course covers all the required steps for working as a doctor in Australia if you are a trainee doctor from Ireland, the UK, US or Canada.
The Competent Authority Pathway. The Option For Trainee Doctors from the UK, Ireland, Canada and USA
If you are a trainee doctor (or Prevocational Trainee) in the UK, Ireland, Canada or the USA. Then you are looking at the competent authority pathway for working in Australia.
The competent authority pathway assigns a preferential status to any doctor who has completed their primary medical training in one of the following countries: the United Kingdom, Canada, the United States, and the Republic of Ireland.
The Competent Authority Pathway. A Possible Option for IMG Doctors from the UK, Canada and USA
In addition, if you are an international medical graduate and you have achieved general registration in the United States, Canada, or the United Kingdom (but not the Republic of Ireland), you may also be eligible for the competent authority pathway.
What are the steps involved in the competent authority pathway?
You can find out more about the competent authority pathway on the Medical Board of Australia website.
The key steps for the competent authority pathway are as follows:
- Securing an employment offer.
- Applying to the Australian Medical Council for primary source verification.
- Applying for registration to the Medical Board of Australia.
- Completing 12 months of supervised practice.
- Applying again to the Medical Board of Australia for general registration.
Eligibility for Competent Authority
You can do a “self-assessment of your eligibility for the competent authority pathway on the Medical Board of Australia website here.
The essential Competent Authority pathway requirements for graduates of UK, USA, Canada, Ireland are.
You need to be a graduate of a medical course conducted by a medical school in one of the Competent Authority countries
AND
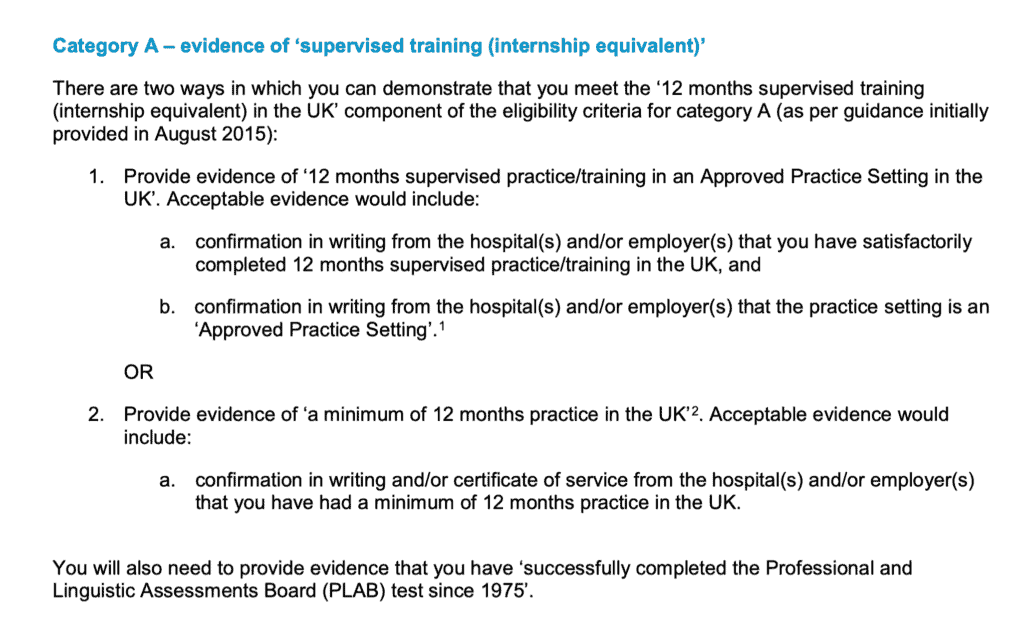
Successfully complete the experiential component required in that country. It is a requirement that this experience is in a supervised position. For the UK, Canada and Ireland you need a minimum 12months supervised experience. For the United States, you need a minimum of 2 years.
The essential Competent Authority pathway requirements for IMGs who have qualified in UK, USA and Canada are.
You need to have completed the AMC Certificate equivalent in the UK, USA or Canada. So the PLAB or the USMLE or the LMCC. You must complete all steps of this qualification.
Plus
Successfully complete the experiential component required in that country. It is a requirement that this experience is in a supervised position. For the UK, Canada and Ireland, you need a minimum of 12 months of supervised experience. For the United States, you need a minimum of 2 years.
No, the MRC… Does Not Count. Nor does just getting registered.
For this reason, doctors who have completed medical school in another European Union country are often unable to register in Australia via working in the United Kingdom as they are usually not required to complete the PLAB. Similarly, many doctors for Gulf State and Asian countries meet one of the multitudes of Royal College exams in the UK and are able to gain registration in the UK without needing to complete the PLAB. Unfortunately, skipping the PLAB means that you are not eligible for the Competent Authority Pathway.
What about the UKMLA?
There is no word yet from the Medical Board of Australia about the United Kingdom Medical Licensing Examination. But I would expect that this would be recognised.
What types of jobs can I apply for as a Competent Authority Pathway Trainee?
You can pretty much apply for any sort of trainee job. There are often a number of postgraduate years 2 or 3 general jobs on offer. They have generally termed Resident Medical Officers in most States and Territories, but may also be called House Officers or Hospital Medical Officers in some places.
Above these sorts of posts come specialty training positions. Australia’s specialty training system is pretty much parallel with the United Kingdom. So you tend to enter specialty training around postgraduate year 3. These positions are generally referred to as Registrar positions. But you might also see them advertised as Senior House Officer or Trainee or Advanced Trainee.
One key thing to look out for is that most of these jobs will not accept an overseas applicant.
A key thing to look for is the phrase “eligible for registration” in the selection criteria.
It is very important to try and secure an employment offer. Whilst you can apply to the Australian Medical Council to check your primary medical degree at any stage. You won’t be able to gain registration until you have an offer of employment. This is because the Medical Board needs to see a supervision plan from your employer.
Outside of general practice, the majority of employment opportunities for trainee doctors occur within public hospitals. So your best places for finding suitable job postings are on the State and Territory health department recruitment sites. We have a listing of these on our international doctors’ resource page.
What Type of Supervision Do I Need Or Get?
The Medical Board of Australia is very vigilant around supervision standards for IMG doctors. What sort of supervision you receive will depend on several factors, including:
- Your qualifications
- Your previous experience, especially in the type of position for which you have applied
- Whether you have practised recently and the scope of your recent practice
- The requirements of the position, including the type of skills required for the position
- The position itself, including the level of risk, the location of the hospital or practice and the availability of support (supervisors)
- The seniority of the position for a hospital position
In general, you will either be approved for Level 1 or Level 2 Supervision. There are 4 Levels, and the higher up you go, the less direct oversight you require.
Level 1 Supervision.
Level 1 Supervision requires your supervisor (or alternative supervisor) to be present in the hospital or practice with you at all times, and you must consult with them about all patients. Remote supervision (for e.g. by telephone) is not permitted. This type of supervision is generally recommended when you are very junior yourself or entering a junior role with which you are not very familiar. In Australian major public hospitals, there are many layers of other doctors from who you can get supervision. So Level 1 is not too much of an issue in these circumstances.
Level 2 Supervision.
Level 2 Supervision, which most competent authority trainees approved to work in Australia will usually be approved for. Level 2 is a step up from Level 1 Supervision. Supervision must primarily be in person, but your supervisor can leave you to do work on your own, and you can discuss by phone. You should consult with them on a regular (daily) basis about what you have been doing with patients. But do not need to discuss every case.
Level 3 Supervision.
Level 3 Supervision is what you might receive if you are working in an Advanced Trainee role in the UK and transferring to something similar in Australia. In this case, you have much more primary responsibility for the patient. Your supervisor needs to make regular contact with you but can be working elsewhere and available by phone or video.
What happens after I commence my position?
Once you are approved for registration, and you have your visa issues sorted, you will be able to commence work. Generally, your employer helps you out with all these things. You will be working under “provisional registration” by the Medical Board of Australia.
Generally, all you need to do for these 12 months is to pay attention, show that you can learn and grow and get regular feedback from your supervisors. Your supervisors will need to complete regular reports for the Medical Board of Australia, and it is your responsibility, not theirs, to see that they are completed and returned on time. If all the reports go well you can be recommended at the end of the 12 months for general registration.
You will probably be looking for another job or negotiating an extension around this time. With general registration, you may be able to apply for a skilled visa and look at applying for permanent residency.
Permanent residency is crucial for applying for some specialist training programs. See below.

Specialist Pathway Course
Free Course
You can enrol now in this free course that will step you through all the requirements for working as a specialist doctor in Australia
The Specialist Pathway. The Option For UK, USA, Irish and Canadian Specialists
For Competent Authority Pathway country specialists, your option for working in Australia is called the Specialist Pathway.
Once again, this starts with becoming verified as a doctor with the Australian Medical Council and should again coincide with an active search for a position.
You may be lucky enough to be in a targeted specialty area where you might successfully be approved for what is called an Area of Need position, in which case the employer or recruitment agent will provide you with a lot of support and will likely pick up the costs of being assessed.
However, Area of Need is becoming extremely rare these days, and I don’t advise actively looking for such a post as you will likely waste lots of time.
For most International Doctor specialists, you will approach the college directly to be assessed for specialist recognition. This is not something to be trifled with. The paperwork requirements and the cost (generally around $10,000 AUD or more) are considerable.
On the plus side, the colleges all have reasonably helpful information on their websites, including the application forms and a little bit about their criteria for assessment.
The Key Steps for the Specialist Pathway Are As Follows:
- Apply to the Australian Medical Council for primary degree and postgraduate degree source verification
- Apply to the relevant college for a comparability assessment.
- Apply for a suitable job offer.
- Apply for registration with the Medical Board of Australia.
- Complete 12 to 24 months of supervised practice +/- examinations.
- Applying again to the Medical Board of Australia for specialist registration.
Finding Out What You Need To Do.
We have saved you the trouble of finding those pages by putting them on our International Doctors resource page here.
The majority of UK specialties (but not all) map to a similar college or specialty in Australia. This is similar for Ireland and Canada. The United States has a more complex arrangement of specialties and subspecialties. But generally working out which specialty goes into which Australian college is generally not too confusing. We have put together a summary of the Australian specialist medical colleges here.
After you go through your specialist assessment, you are given an outcome.
In most cases for Competent Authority specialists, you will be deemed substantially comparable. This essentially means that you will need to work under some form of peer review for up to 12 months and so long as your reports are satisfactory, you will be recommended for specialist registration at the end.
Occasionally Competent Authority Pathway specialists are deemed to be partially comparable (a situation where this may occur is if you have just recently finished specialty training but have not worked as a specialist for very long). In this
Rarely are Competent Authority country specialists deemed not to be comparable by the college. This only happened to 6 out of 409 UK doctors in 2017 (less than 1%). If you are deemed to be not comparable, this means you cannot directly become a specialist in Australia. You will probably have to go through the competent authority route and re-enter training in Australia.
How to Maximize Your Chances of Getting a Substantially Comparable Outcome.
To ensure that you are seen as substantially comparable by the relevant college, I would recommend the following:
- You should have your Certificate of Completion of Training and relevant college Fellowship for the UK or equivalent for other countries e.g. Board Certificate for the US.
- You should ideally have worked substantively at a Consultant level in your field for 3 years or more
- You should be able to demonstrate good standing with your medical board and your employers
- You should be able to demonstrate ongoing continuing professional development
- You should prepare for your interview with the college as if it were an important job interview
Can you enter training in Australia if you are a Competent Authority Pathway doctor?
To undertake formal specialty training in Australia you need to be accepted into a college training program. In all circumstances, you will need general registration and in many cases permanent residency or citizenship.
After receiving your general registration Competent Authority pathway doctors can apply for specialty training in the same way that Australian-trained doctors do. And if accepted will go through the exact training program and experience. Some colleges may offer some recognition of prior learning that you have done already. But this is often quite limited and may at best normally shave one year from your training.
Can you do your internship in Australia as a UK, US, Irish or Canadian doctor?
Basically no. Internship in Australia is a provisional year that only applies to medical graduates from medical schools in Australia and New Zealand. There is a “loophole” that only applies to doctors who have not been able to complete an internship or equivalent in their own country. But the Medical Board warns that this is not a great option and is only granted in limited cases. You are far better off applying for the Foundation Program in the UK and completing at least Foundation Year 1, completing the Internship program in Ireland, completing 1 year of residency in Canada or 2 years in the United States.
How many Competent Authority doctors are working in Australia?
There is no one public data source to tell us how many Competent Authority doctors are currently working in Australia.
From data collected by the Australian Government, we know that for trainee doctors for 2018:
- 639 applications were made for provisional registration via the competent authority pathway by UK doctors with 623 granted provisional registration.
- An additional 36 applications were made for provisional registration via the competent authority pathway by doctors who had completed the PLAB in the UK, with most of these also being granted provisional registration.
- 263 applications were made for provisional registration via the competent authority pathway by doctors from Ireland with 257 granted provisional registration.
- 40 applications were made for the competent authority pathway by US doctors with 30 granted provisional registration through that pathway.
- 21 applications were made for registration under the Competent Authority Pathway by Canadian doctors with 20 being granted.
How hard is it to become a specialist in Australia if you are from a Competent Authority country?
Specialist doctors from the competent authority countries are not automatically granted specialist recognition. However, most are. For example, in 2019 there were 430 applications made for specialist assessment to the Australian colleges by UK doctors and of these, the majority were deemed substantially comparable.
UK doctors tend to get a very
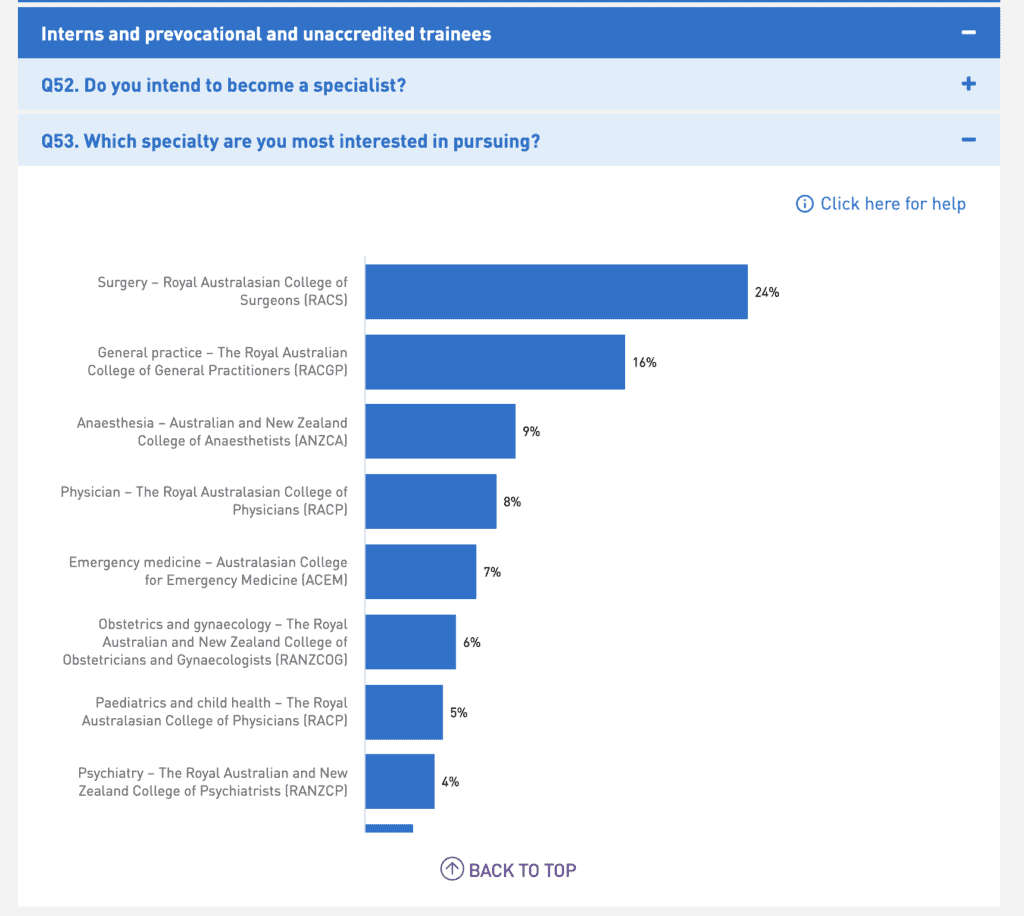
Are there any particular specialties that are easier to apply for?
The majority of specialties have some vacancies and will provide opportunities for Competent Authority IMG doctors from time to time. This is particularly the case if you are prepared to go outside of the major cities. Some areas of medicine are more popular and so finding jobs in areas such as most surgical fields, as well as other fields such as cardiology can be pretty difficult.
On the other end of the spectrum general practice, psychiatry, and most parts of critical care medicine are often always looking for doctors.
Costs of Moving To Australia and Working As a Doctor.
There are many costs to consider when considering moving to Australia to work as a doctor.
There are some direct costs to consider. Most relate to the bureaucratic process of being assessed and gaining registration.
Some of the costs you may be up for include:
| AUD (unless otherwise noted) | |
| Establish a Portfolio with the Australian Medical Council | $600 |
| Registering with EPIC and having one primary degree checked | $130 USD + $100 USD |
| Medical Board Application Fee for Provisional Registration | $430 |
| Medical Board Application Fee for Specialist or General Registration | $860 |
| Medical Board Provisional Registration Fee | $430 |
| Medical Board General or Specialist Registration Fee | $860 |
| College Specialist Assessment Fees* | $7,000-$15,000 |
| College Placement Fees (for a period of supervision)* | $8,000-$30,000 |
*Only applicable to Specialist Pathway
Compared to the regulatory costs for other pathways, the Competent Authority Pathway is quite cheap.
The Cost of Your Time and Effort.
To all of this cost, you will need to factor in the cost of your own time. It takes some time effort and persistence to deal with the paperwork and track down the records you need, particularly for the specialist pathway.
In addition, you will probably have to pay costs in your own country for things like records of schooling and certificates of good standing.
There are also visa costs.
And then there is the cost of airfares and transporting your belongings halfway across the world.
Depending on where you work in Australia, you may find that the cost of living is higher or lower than you are used to. House prices and therefore house rental rates have gone through the roof in Australia in the last decade or so but are starting to come down.
You will probably have to factor in some initial extra hotel or short-term rental charges whilst settling in, and you may find if you have children that you have to pay to enrol them in school as public schooling is only generally free if you are a citizen or permanent resident.
If you are lucky and in one of the specialty areas of demand, your employer may offer to pay for some of these costs. It’s certainly worth asking about it.
Related Questions.
Why do UK doctors move to Australia?
Are there other options for working as a UK doctor in Australia?
Should I use a medical recruitment company if considering working in Australia?
How much do doctors earn in Australia?
The cost of living in Australia is generally on a par with that of living in the other competent authority countries.
Salaries also differ in Australia depending on the state or territory. But generally, an intern (PGY1 or FY1) earns between $70,000 and $80,000 AUD baseline salary in Australia. After completing the internship your salary will vary somewhere between $80,000 to $160,000 AUD as you progress through your training.
Consultant salaries in Australia can be quite considerable.
GPs earn the least but still generally manage to earn over $200,000 AUD if they work full time and some specialties can earn as much as $600,000 AUD on average.
What is the Australian equivalent of the GMC (General Medical Council)?
You would think that by virtue of its name the Australian Medical Council is the same as the GMC. But it is not. The AMC accredits medical training insitutions such as medical schools and specialty colleges as well as some aspects of the verification of IMG doctors.
The Medical Board of Australia is responsible for the registration process as well as reviewing maintenance and upholding of standards, dealing with complaints against doctors and reviewing their performance if needed.
The competent authority pathway really belongs to the Medical Board. It is not really an AMC competent authority pathway.
How do I become an IMG in Australia?
Can I work in Australia with GMC registration?
I qualified in New Zealand under the NZREX. Am I eligible for the Competent Authority pathway?
I completed an Osteopathic Medicine program in the United States. Am I eligible for the Competent Authority pathway?
You are required to complete all phases of the Comprehensive Osteopathic Medical Licensing Examination (COMLEX-USA) as well as a minimum of 2 years of graduate medical education in a residency program accredited by either the ACGMR or American Osteopathic Association.