Based On An Article Originally Requested By the NSW Medical Students Council about medical student resumes.
Being able to compile a CV or Resume is an essential skill for pretty much any career. But as a medical graduate, you may not necessarily have been taught this specific skill so far.
In my experience it is uncommon for medical schools in Australia to cover how to compile a medical student resume as part of their formal curriculum. But that’s okay. It is a skill that you can actually teach yourself with a bit of research and guidance. I’ve reviewed tens of thousands of CVs and Resumes in my time and helped hundreds of doctors write or rewrite their resumes. So, you are in good hands.
Unique to the state of New South Wales, where I reside, the only medical graduates who need to put a resume together are those applicants applying for Rural Preferential Recruitment (RPR). This is because this is the only pathway that employers are directly involved in the selection process. So, I am pleased to have been invited to write this article specifically for that purpose. But even if you are not applying for RPR you will probably learn something by reading this article because you will definitely need a resume in the next few years.
Let’s start with the basic features of your medical student resume, which components are most important, and the recommended order. After which I will go into some more detail about 3 key aspects of your resume that are important to consider when applying for a rural internship (your personal statement, describing your education and choosing your referees).
The Basic Medical Student Resume Format
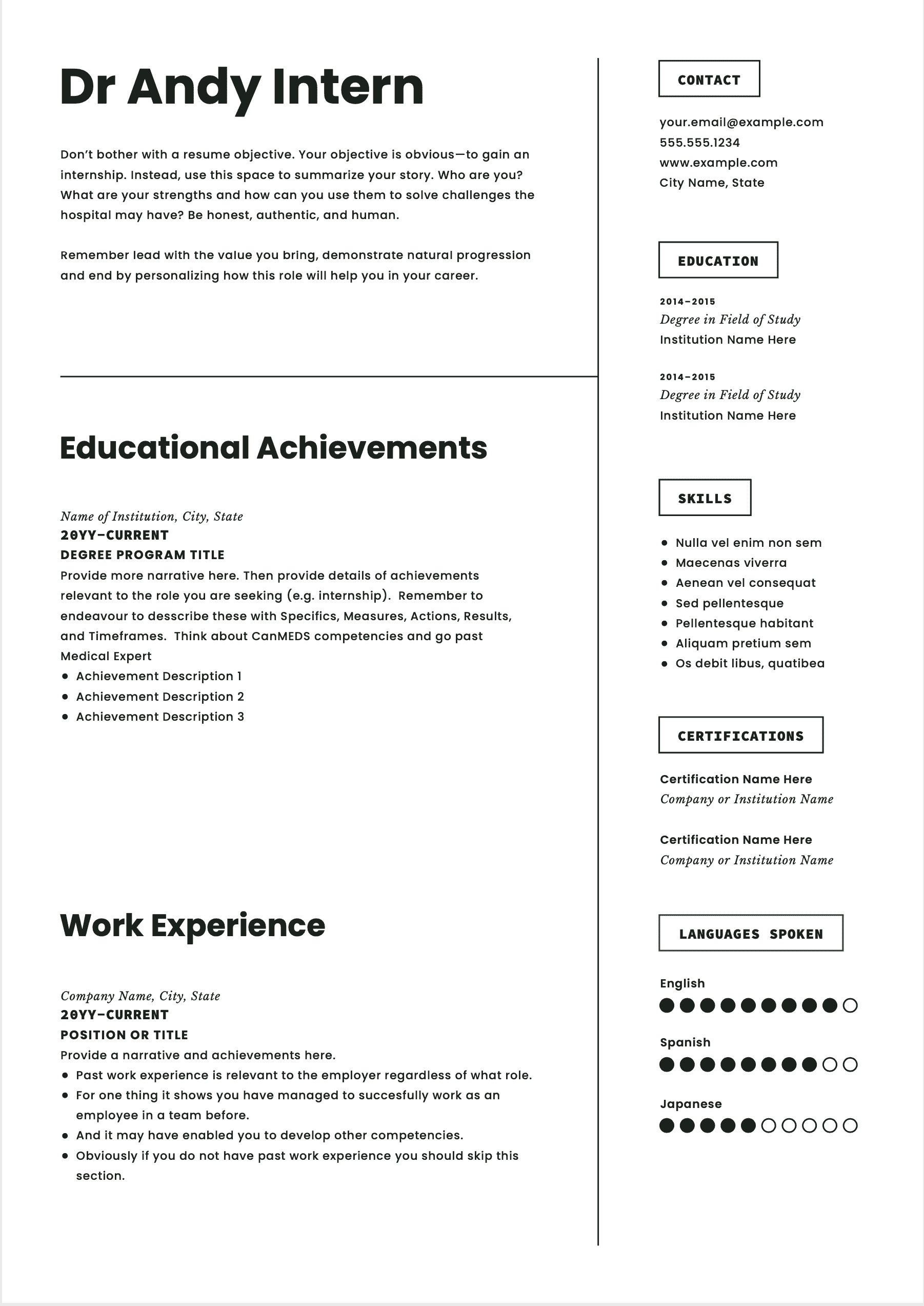
Included in this article is an example of how you can put together a 2-page medical student resume for your internship application.
You can also download this as a word doc template from the following link [will provide you the link].
Most medical graduates will only need 2 pages for their medical student resume. But honestly if you need to go to another page or two that is fine. Just know that when your CV is reviewed the first time, its not reviewed for very long (about 8 seconds) and most of that time is spent reviewing what is on the first page. So, you need to be circumspect about what you do and don’t include on this page.
The Front Page
The front page of your medical student resume and in fact the top third of the front page is where you need to put down all the essential information that you absolutely want the employer to see and acknowledge. You will notice in the example above the biggest element on the front page is the candidate’s name. That’s deliberate. That’s the one thing you want them to remember the most. You notice I have also put Dr as a prefix. Now you may not feel comfortable doing this if you have not officially completed your degree yet. If so. That’s OK. But definitely include it in future resumes. It displays confidence and formality.
You will also notice that high up on the front page of this medical student resume are some basic details, including your contacts (you want the employer to be able to contact you easily) and your short qualifications. For medical jobs there are some essential requirements for most jobs. These include items like having a medical degree, having the appropriate registration, and in some cases things like being registered with a college, having English language proficiency, and eligibility to work in Australia are also important. So, all of these should be high up on the front page so that they are seen, and the employer can tick the necessary boxes.
You will see that the other prominent element in the top third of the medical student resume is a statement. We generally refer to this as a personal statement or career goal statement. I recommend spending some time on getting this piece of text right. It should provide a compelling story for the reviewer to want to talk to you in person. But do this last after you have put together all the other elements of your resume as you will want to draw on some of these. More about the personal statement shortly.
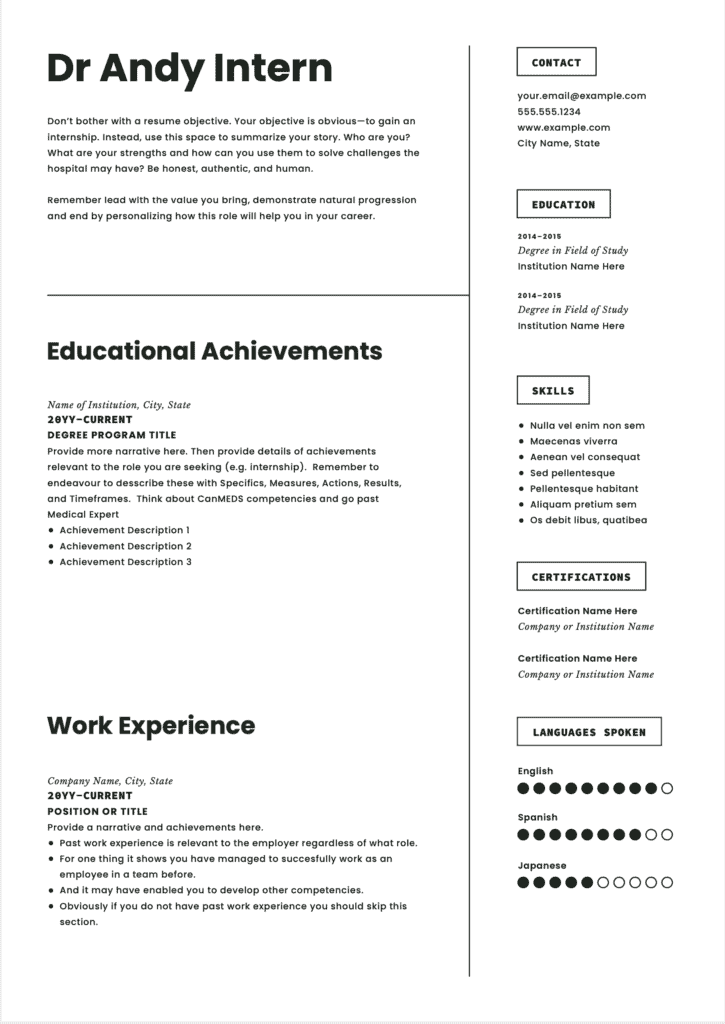
For most medical student resumes work history comes straight after the personal statement. Employers are most interested in what you have been doing in your most recent job.
For medical graduates however your most recent significant activity has been your education, so this comes next and this provides yet another opportunity to describe some of the things you have been doing and most importantly have achieved.
If you do have work history, it’s a very good idea to include some information about this as a bare minimum it demonstrates that you have been employable in the past and in most cases demonstrates many more things about you.
What Other Headings Should You Use on Your Medical Student Resume?
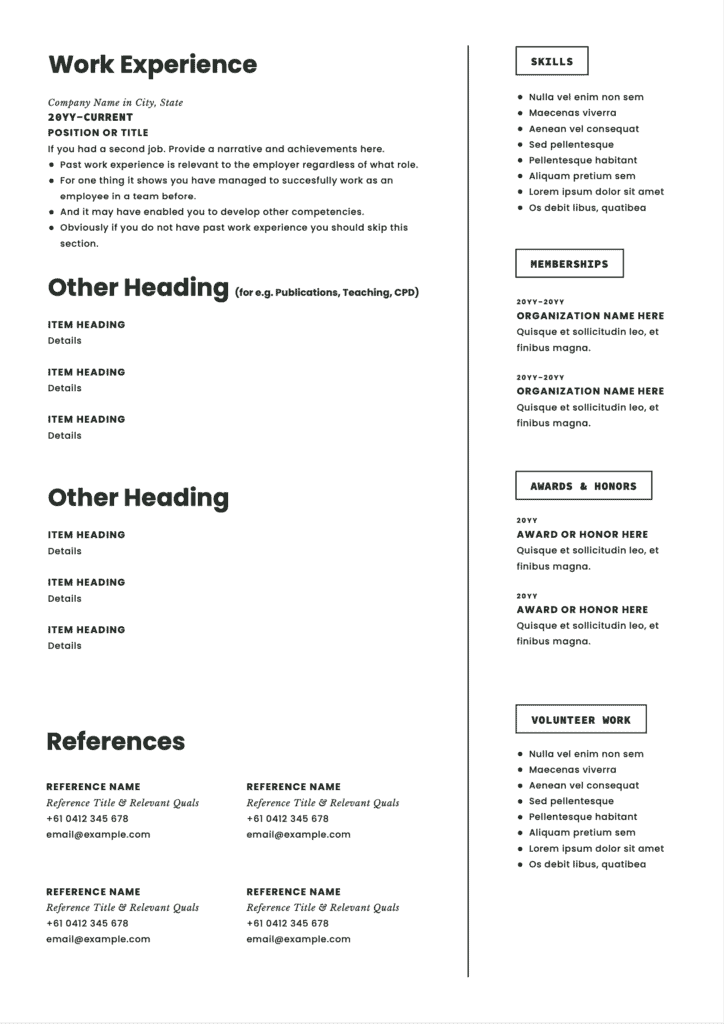
You will see that I have suggested a range of other headings that you can use both in the short right hand column and after work history. Other than work and education there is no set rule as to what you should include and where in your Resume. I would recommend including the next thing that shows your strengths. So if this is your teaching experience talk about this next. Or if it is the fact that you have already done some decent research, talk about this.
The only caveat to this is that referees always come last on the resume.
Needing More Help With Your CV or Resume
We have plenty of options from a premium online CV builder to expert editing and advice.
3 Specific Areas to Focus In Your Medical Student Resume For a Rural Internship
Picking appropriate referees, describing achievements and writing a compelling personal statement are key to all resumes. Let’s talk about how to make them relevant in your resume application.
Referee Selection
When I speak to medical students about the need to have referees on their resume, they often get caught up in the need to have well-known consultants as referees on their resume.
This is not the case. And often times your exposure to brand name consultants who really get to know you is limited anyway.
It’s more important to focus on a having a diverse range of referees that have recent and relevant knowledge of you.
A mixture such as a consultant, a registrar and a Nurse Unit Manager or even a professional staff member from your medical school is generally fine. But try to ensure that there is at least one female and one female on your list. And aim for at least some of these people to have had decent exposure to you in the last 12 months or so.
In terms of relevancy for a rural internship, it may seem an obvious point but having people listed who work in rural areas is going to go a long way in terms of your candidacy. Here’s something that you probably don’t know. The rural hospitals in NSW that take internships have strong networks with each other. The JMO Managers and Directors of Training at these hospitals generally know each other on a first name basis. This network also usually extends to local clinical school staff. So, if you are able to put someone like a Clinical Dean on your resume this will go a long way for you.
Educational Achievements
One of the more tedious parts to read of most doctor resumes is their work history and education history. It’s almost 99% a list of rotations and responsibilities, which says nothing about how they actually performed.
By all means give a quick summary of where you were for each of your years of medical school. But quickly focus in on the things that you particularly did that prove that you are suited for a rural medical career. There are some obvious candidates here, such as spending a year at a rural clinical school or being a member of a rural club.
Less obvious might be parts of your course where you focused on generalist medical skills and methods of delivering health care.
If possible, list at least a couple of things under your education history that show you can get things done. This does not necessarily need to directly link to rural health. But is a bonus if it can. I like the SMART acronym for this.
Try to describe your achievement end ensure you are Specific about what your achievement was. That you can Measure the success of your achievement. That you can describe your specific Actions in that achievement. And that you can describe the Result and Timeframe in which it occurred.
So, here is an example that demonstrates SMART,
“In my final year of medical school, we were set a group task to deliver a presentation on the differences between urban and rural mental health outcomes. I noticed that we were having some initial trouble as a group in developing individual roles and accountability. So, I volunteered to act as the secretary of the group to ensure better coordination of group roles and tasks. This had an almost immediate effect on improving group dynamics and ultimately contributed to our group delivering the project ahead of time, gaining a higher distinction for our project and being selected as one of two groups to present our findings at the end of the year.”
You will notice that the example doesn’t really touch much on medical knowledge or skills, but demonstrates skills and values such as emotional intelligence, professionalism, and a desire to achieve success as part of a team. These are all highly desirable characteristics for employers.
In terms of competencies that you could demonstrate in your resume I recommend you review the CanMEDS framework [http://www.royalcollege.ca/rcsite/canmeds/canmeds-framework-e] for further inspiration.
Personal Statements
Finally, we come to the personal statement. There is a lot to personal statements. So if you want to explore them more fully I have written more about the topic on the AdvanceMed Blog (advancemed.com.au). However, I think for rural preferential internship there are 2 unique ways to go with your personal statement.
Some of the medical graduates applying for rural interest will be from a rural background and the remaining will have an interest in rural health.
For the first group. Those with a rural background. This is a strong selling point. The evidence around rural background and the rural training pipeline is well-known to rural hospitals and they are actively seeking candidates from this group as they know they have a high chance of becoming more permanent than just completing a year of internship and residency. So, it’s definitely worth weaving this into your personal statement.
My general formula for the personal statement is to:
- Offer some value to the employer.
- Show natural progression.
- Demonstrate how the opportunity helps you.
So, for graduates from a rural background you can easily weave your background in at points 2 and 3 of this formula. In which case you can if you want talk about one or two other key strengths for points 1.
For example,
“I bring 4 years of high-quality medical school training with a strong emphasis on communication and teamwork schools, I was also awarded a prize for my academic prowess in the area of surgery. Having been born and high-schooled in a rural NSW town and spent 50% of my medical school at a rural clinical school, I am very prepared and excited to commence my internship at a rural hospital. A rural internship will also help me with my longer-term career aspiration to be a rural general surgeon.”
For graduates who do not have a rural background but are interested in rural health you should take the opportunity to point out that a rural internship is the obvious next step for someone interested in rural health and will help you to define a rural career. But, because you do not have that obvious rural background. I would suggest that its also worth pointing out what specific rural exposure and training you have had so far at Item 1.
For example,
“I have spent the last 2 years of medical school studying at 2 separate rural clinical schools. In that time I had developed a good understanding of the challenges for rural health as well as been able to identify that some of my strengths, such as personal communication and working within small and agile teams, are well suited to working in a rural hospital. My rural hospital experience to date means that I am well prepared to take on a rural internship. Further a rural internship will greatly assist me in my desire to one day become a rural general practitioner.”